INTRODUCTION
Average life expectancy has consistently been increasing worldwide, having reached over 70 years by 2015 [1]. This extension of life span has been associated with more rigorous health checks and an increasing incidence of early breast cancer in older patients [2,3].
In the past, elderly with breast cancer frequently underwent conservative treatment only for breast cancer. Although breast cancer grows more slowly and has a better prognosis in elderly [4,5], many studies have suggested that they should be managed actively [6-10]. However, the comorbidities of elderly may hinder implementation of active forms of treatment.
The American Society of Anesthesiologists (ASA) Physical Status classification of surgical patients is a standard element of preoperative assessment [11]. Although this classification does not propose absolute criteria for suitability for general anesthesia, an individual’s risk of postoperative complications or morbidities can be predicted because the presence and severity of comorbidities have been evaluated. When a patient has an extremely high risk of postoperative morbidity or mortality, the patient and their caregivers may refuse surgery under general anesthesia not because they believe that the surgery itself is too dangerous, but because they fear life-threatening postoperative complications of general anesthesia.
Surgical removal is the most important treatment for breast cancer regardless of whether other neoadjuvant or adjuvant treatments are administered [12,13]. Excision of breast cancers not only reduces tumor burden, thus maximizing the therapeutic effect, but also enables accurate assessment of tumor characteristics, which is important when considering adjuvant treatments. Removal of the main lesion is important as treatment of breast cancer that consideration should be given to performing it under procedural sedation in elderly who are at high risk of complications after general anesthesia. However, there is no remarkable oncologic result according to the anesthetic method which makes the type of surgery differently.
This study was conducted to assess the efficacy and safety of performing surgery for breast cancer under procedural sedation in older patients when general anesthesia is considered too risky.
METHODS
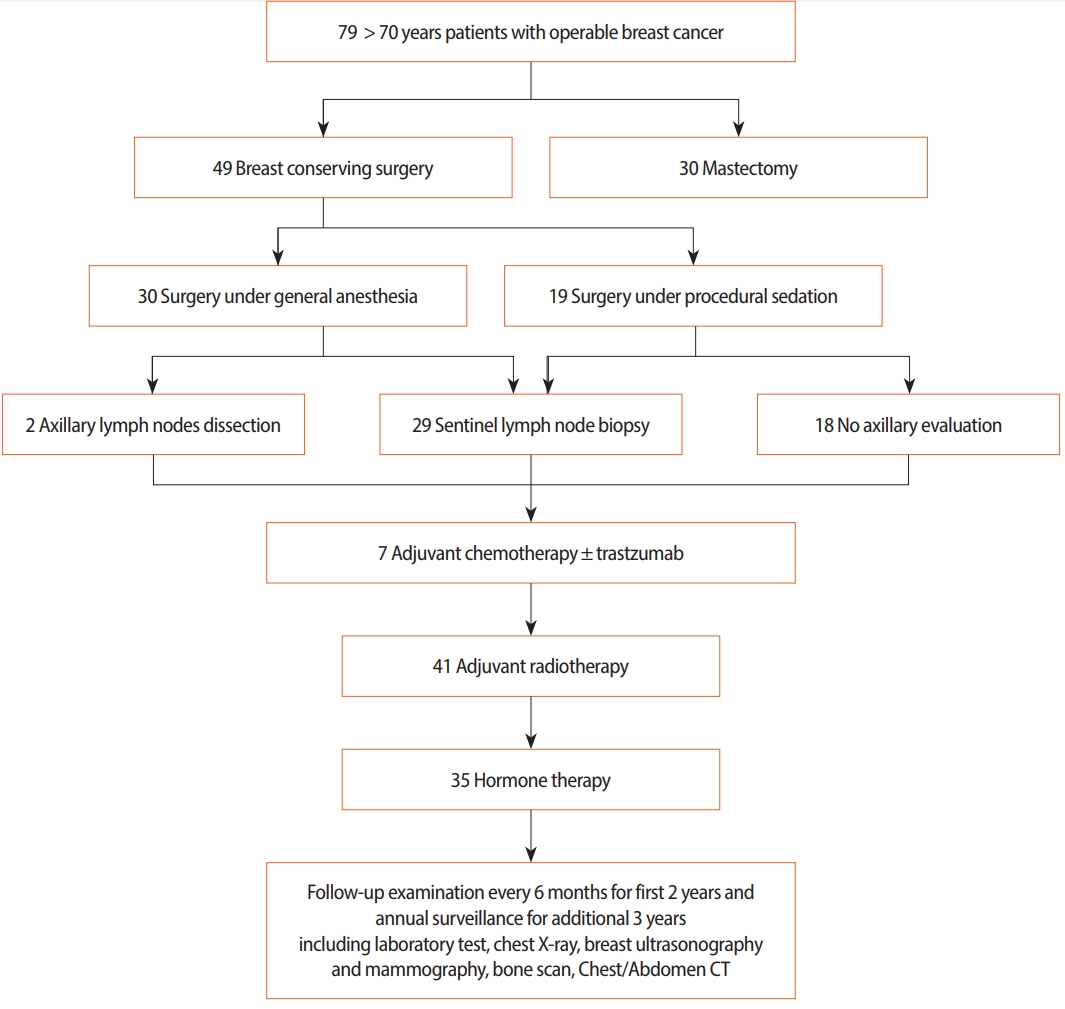
Data of 79 eligible patients with operable breast cancer who were older than 70 years and attended our institution between January 2011 and December 2016 were collected prospectively for this study. Of these, 49 patients underwent breast-conserving surgery under general (n=30) or procedural sedation (n=19). These patients’ clinical and oncologic factors were compared and analyzed (Figure 1). The study protocol used was approved by Institutional Review Board at the Kyungpook National University Chilgok Hospital.
All breast cancers were confirmed by core needle or excision biopsy and their size, number and location assessed by mammography, ultrasonography, and breast magnetic resonance (MR) imaging. The axillary lymph node was negative in all patients based on imaging modalities. Patients with severe heart disease or pulmonary condition that precluded them being in a prone position for 40 minutes did not undergo breast MR. And the results of preoperative blood tests, chest X-ray films and electrocardiograms were used to determine the patients’ ASA physical status.
Informed consent for surgery and anesthesia was obtained from all patient and their caregivers by surgeons or anesthesiologists who explained the predicted risk of postoperative complications. A surgery under procedural sedation was decided for the patients and their family who refused general anesthesia because of high risk of postoperative morbidity or mortality. Among them, only one case was performed an axillary evaluation as sentinel lymph node biopsy.
General anesthesia was performed according to our institution’s standards as either a balanced (BAL) or totally intravenous anesthetic technique using target controlled infusion (TCI). Patients were monitored throughout the procedure by measurement of BP, heart rate, peripheral oxygen saturation, electrocardiogram, bispectral index (BIS), end tidal desflurane, and end tidal CO2. In the patients undergoing TCI, anesthesia was induced with continuous propofol and remifentanil infusion (OrchestraⓇ with Base Primea; Fresenius Kabi, France) to reach 3–4 μg mL−1 and 2–4 ng mL−1 of target effect-site concentration (Ce). In those undergoing BAL, anesthesia was induced with propofol 2 mg kg−1 and continuous remifentanil infusion, using TCI to reach 2–4 ng mL−1 of Ce. All patients were intubated and ventilation was adjusted to maintain an end tidal CO2 between 30 and 35 mmHg throughout the surgery. BIS values were used to guide administration of propofol and desflurane. The target range of BIS during maintenance was 40–50. Mean arterial pressure and HR were used to guide administration of remifentanil, the aim being to maintain them within 20% of preoperative values. At the end of surgery, neuromuscular blockade was reversed with pyridostigmine and glycopyrrolate (0.2 mg/kg and 0.008 mg/kg, respectively).
Procedural sedation was performed with intravenous injection of a sedative (MidazolamⓇ Bukwang Pharm, Seoul, Korea) and analgesic agent (PethidineⓇ Jeil Pharmaceutical Co. Ltd., Daegu, Korea) and monitored by surgeons themselves. Patient was placed in the supine position with both arms abducted and a peripheral capillary oxygen saturation (SpO2) was measured with a pulse oximeter during surgery. The intravenous agents were administered as 5-mg of MidazolamⓇ mixed in 100-mL of normal saline, started at the time of breast draping in 60 gtt/minute and 50-mg of PethidineⓇ mixed in 100-mL of normal saline, started at the time of surgical incision in 12 gtt/minute. Before the surgical incision was initiated, 2%, 5-mL of LidocaineⓇ was injected on subcutaneous layer. When the patient feel operative site pain, the 2% of Lidocaine was more injected or IV rate of PethidineⓇ was raised.
Conventional breast-conserving surgery or mastectomy was performed, the surgical margins being evaluated after breast-conserving surgery by intraoperative frozen section. When a surgical margin was found to be positive, additional resection was performed until the surgical margin was confirmed as tumor-free. Sentinel lymph node biopsy (SLNB) or axillary lymph nodes dissection (ALND) was performed according to axillary lymph node status.
Although the main breast lesion was widely removed to achieve safe margins, surgical margins were not evaluated by frozen section in patients undergoing procedural sedation. Additionally, SLNB was rarely performed in the procedural sedation group because of pain and time limitations. Postoperative adjuvant treatments were administered according to tumor stage, hormone receptor status, and HER2 gene positivity.
Various clinicopathologic variables including age, body mass index (BMI), underlying disease, length of hospital stay, duration of fasting, ASA physical status, bilaterality, tumor location, type of surgery and anesthesia, duration of follow up, and oncologic results were analyzed. Pain was assessed immediately postoperatively on a visual analog scale (VAS) [14]. All variables were compared between the general anesthesia and procedural sedation subgroups of the breast-conserving surgery group. The statistical significance of differences in variables between groups was performed using the χ2 or Student’s t-test for categorical and continuous variables, respectively.
RESULTS
The overall mean age was 75.6 years (±SD, 4.11) and mean BMI was 23.1 kg/m2 (±SD, 2.79). Among them. 47 patients (59.5%) had hypertension, 35 (44.3%) patients had diabetes mellitus, 16 (20.3%) patients had various forms of heart disease, and 4 (5.1%) patients had been diagnosed asthma.
As to ASA physical status, 58 patients (73.4%) were classified as Class II and 21 (26.6%) as Class III. Depending on tumor size, 30 patients (38.0%) had undergone mastectomy under general anesthesia and the remaining 49 had undergone breast-conserving surgery under general (30 patients; 38.0%) or local (19 patients; 24.1%) anesthesia. The mean duration of follow up was 36.6 months (±SD, 6.04). One patient had developed a local recurrence in the axillary area (Table 1).
The mean age was significantly younger in general anesthesia group (p=0.014) and more patients had grade III ASA physical status in procedural sedation group (p=0.035). The mean operation time and hospital stay shorter in the procedural sedation group (p=0.024, p<0.001). Only one patient in the procedural sedation group underwent evaluation of axillary nodes. Pain scores tended to be higher in the general anesthesia group; however, mean pain scores immediately postoperatively did not differ significantly between the two groups (p=0.076). Even if the axillary evaluation was not performed in procedural sedation group except one case, three patients received adjuvant chemotherapy due to triple negative breast cancer (n=2) and HER2-positive breast cancer (n=1) (Table 2).
There was only one case of local recurrence in patient who was received breast conserving surgery with sentinel lymph node biopsy under general anesthesia. However, any metastasis or death was not occurred during follow-up period. And there was no significant difference of pathologic characteristics between two groups and the oncologic results, also, did not show statistical significance between two groups (Table 3).
DISCUSSION
Geriatric patients differ from younger patients in that they are more likely to have multiple comorbidities and their vital organs are less robust [15]. Breast cancer usually grows more slowly in older than younger patients and has a better prognosis and higher rate of hormone receptor positivity [16-19]. Although all patients with breast cancer, including older patients, should be treated according to standard treatment protocols, older patients are frequently under-evaluated or under-treated because of comorbidities, insufficient socio-economic support, or the decisions of their caregivers [6,20].
Surgery is the most important modality for treating breast cancer disease and achieving optimal outcomes and is generally supported by adjuvant treatments [21-23]. These general principles hold true for elderly. Surgery for breast cancer is generally performed under general anesthesia and comprises removal of the primary lesion and evaluation of axillary lymph node status. There are several reasons for performing breast cancer surgery, including breast-conserving surgery, under general anesthesia. First, definitive pathologic evaluation of intraoperative margins takes quite a long time. In the case of breast-conserving surgery, the need for any additional excision can be determined by examination of frozen sections. Second, surgery in the axillary area is relatively painful because there are many sensory nerves in this region. Additionally, ALND is more dangerous procedure than breast surgery because it involves exposure of major vessels and therefore requires a meticulous procedure.
When older patients with breast cancer are considered at high risk of perioperative complications after general anesthesia, surgeons must decide whether to give forego surgery or choose another type of anesthesia. Important considerations include the following. A meta-analysis has shown that the results of hormone treatment alone without surgery are inferior to those achieved by surgery with or without hormone treatment [24]. Additionally, because reducing tumor burden is important in treatment of breast cancer, intensive treatment including surgery and chemotherapy is optimal even in older patients.
Elderly patients with breast cancer are frequently received under-treatment for their disease. However, if a tumor burden has been decreased after removal of primary breast cancer, even if the axillary dissection, adjuvant radiotherapy or chemotherapy is omitted, the oncologic outcome was not inferior to conventional treatment of breast cancer [25]. Similarly in the present study, although axillary lymph node status was not assessed in the former, the oncologic results did not differ significantly between the general anesthesia and procedural sedation groups during follow-up. However, the mean hospital stay and fasting time were shorter in the procedural sedation group, which may have assisted postoperative recovery. Additionally, the mean pain score immediately postoperatively was lower in the procedural sedation group. However, because these patients did not undergo axillary surgery, comparison of pain scores is not valid.
Surgical removal of breast cancer under procedural sedation may have advantages over not performing any surgery in patients for whom general anesthesia is assessed as too risky. First, excision decreases tumor burden, enabling maximal therapeutic effects from adjuvant treatment, especially hormone treatment. Second, excision minimizes progression to inflammatory or metastatic breast cancer, resulting in a better quality of life. Third, excision enables more precise characterization of tumors, which is helpful in deciding on adjuvant treatment. Fourth, removal of the tumor likely reduces tumor-related fear and anxiety.
There is little published evidence that procedural sedation is superior to general anesthesia. Sedatives and analgesics should be used with caution in older patients because changes in their body composition and pharmacokinetics can affect the absorption, distribution, and elimination of such agents [26,27]. Moreover, shock or acute heart issues can occur when older persons experience severe pain or stimulation during surgery under procedural sedation. Thus, surgery under general anesthesia may be safer because this prevents any pain or fear intraoperatively.
However, procedural sedation bypasses potential life-threatening complications of general anesthesia. In addition, the recommended perioperative fasting time is shorter for procedural sedation, which minimizes any exacerbations of catabolic states and enables better nutritional support, thus facilitating recovery [28].
There are several limitations. First, the population was small and follow up period was not long. Therefore, even if the authors performed multivariate analysis as well, we could not satisfactory statistical results. Further study would be necessary to analyze more accurate oncologic outcomes for breast cancer. Second, in most case, the sentinel lymph node biopsy was not done which could affect to analysis. In addition, since the surgery under procedural sedation was performed for the elderly patients who had relatively early breast cancer, this could be a bias in analyzing. However, this study is the first study of oncologic data in comparing anesthetic method for elderly patients with breast cancer. And this study shows very optimistic aspect of surgical role in those patients.
In conclusion, a breast surgery under procedural sedation is a safe and effective means of reducing tumor burden in older patients with breast cancer who are considered at unacceptable risk of life-threatening perioperative complications after general anesthesia on the basis of ASA physical status. And the oncologic results of breast conserving surgery under procedural sedation may be not inferior to breast conserving surgery under general anesthesia.