INTRODUCTION
Histologically, the axillary area contains lymph nodes and various mesenchymal tissues, such as skin, fat, muscle, blood vessels, and nerves. As a result, a wide range of diseases can present in the form of axillary masses. Clinically, palpable axillary masses should be distinguished from common causes such as lymphadenopathy, as well as diseases including vascular disease, nerve-origin tumors, and accessory breast tissue [1].
In addition to clinical reasoning, radiologic evaluations such as mammography (mediolateral oblique view), sonography, computed tomography (CT), and magnetic resonance imaging (MRI) must be performed to differentiate these diseases. Additionally, for histological confirmation, a pathological biopsy through fine-needle aspiration, ultrasound-guided needle biopsy, or surgical excision is required [2].
Ectopic breast tissue, which was confirmed in this case, is commonly caused by incomplete regression of the embryonic mammary ridge (milk line) located from the axilla to the groin. Ectopic breast tissue can be distinguished relatively easily if it is present bilaterally or if the areola and nipple are expressed; however, such tissue can often be confused with other diseases [3]. In particular, axillary ectopic breast tissue with a diameter of more than 5 cm is rare, and if it occurs in men, misdiagnosis of other diseases, such as lipoma or liposarcoma, is likely to occur [4]. In this case report, we describe a rare clinical case of a giant unilateral mass of ectopic breast tissue occurring in the axilla of a male patient.
CASE REPORT
A 57-year-old male patient without any medical history presented with a large mass in the right axilla that was palpable for several years prior. The mass started growing rapidly approximately one month prior to his presentation at the clinic. Although no accompanying pain or tenderness was reported, the patient wanted surgical removal of the mass because of discomfort in his daily life due to its large size and hyperpigmentation of the axillary skin (Figure 1). No specific findings were found in the blood laboratory tests. Hormonal tests, including luteinizing hormone, follicle-stimulating hormone, estradiol, and testosterone, were within the normal ranges. Preoperative CT was performed to establish a surgical treatment plan and for differential diagnosis. Based on the radiologist’s findings, a lobulated tumor contacting the skin layer inside the right axillary fat tissue was identified, and a soft tissue sarcoma was suspected (Figure 2).
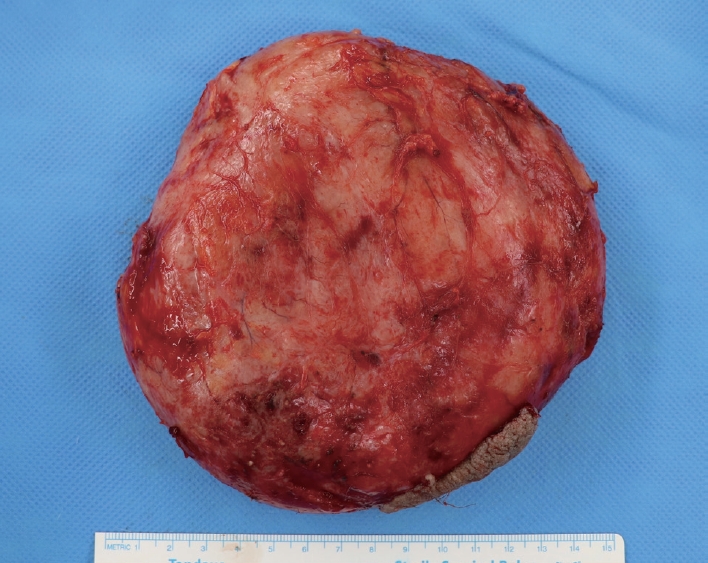
Total excision under general anesthesia and histological evaluation of the mass were performed. A 10 cm incision was made at the center of the mass and dissection was performed. Part of the hyperpigmented skin was resected, and the mass was completely dissected from the surrounding tissue. Total excision of the mass was performed after confirming no damage to the adjacent tissues (Figure 3). As a result, a 15×14×4 cm large mass was extracted (Figure 4).
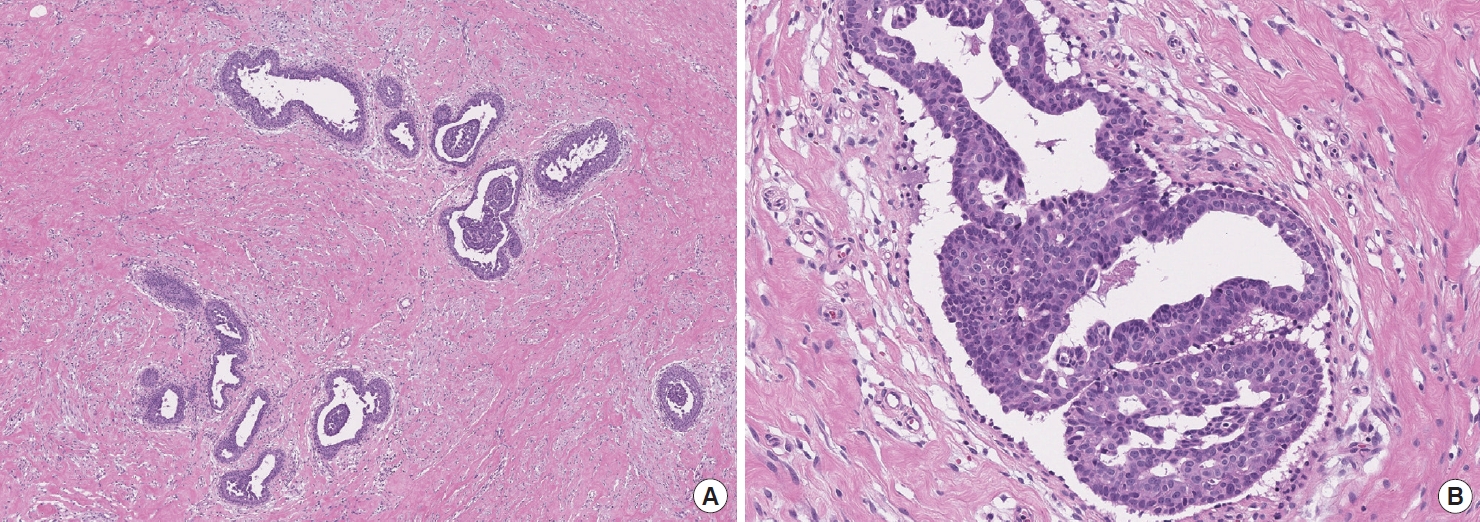
After surgery, histological analysis was performed by a pathologist using hematoxylin and eosin staining. Pathologically, the axillary mass showed ductal epithelial and stromal proliferation and a loose mucosal matrix surrounding the ducts. No other pathological abnormalities were observed in the breast tissue. We determined that there was a very high possibility of pure ectopic breast tissue compared with the possibility of a pure ectopic breast and a newly occurring benign tumor with ductal hyperplasia inside the pre-existing ectopic breast. Consequently, the axillary mass was confirmed to be pure ectopic male breast tissue (Figure 5). During the 3-month postoperative follow-up period, no significant complications occurred, including hematoma, seroma, or recurrence (Figure 6).
This case report was approved by the Institutional Review Board of Inje University Ilsan Paik Hospital, and the written informed consent was obtained from the patient for the use of images.
DISCUSSION
In patients presenting with an axillary mass as the chief complaint, it is preferable to distinguish the mass from unilateral or bilateral axillary lymphadenopathy caused by diseases such as mastitis, infection, collagen vascular disease, and lymphoma. Additionally, masses originating from the breast tissue, including accessory breast tissue; tumors originating from the skin, including axillary tail lesions, epidermal inclusion cysts, and pilomatrixoma; and masses originating from subcutaneous tissue or muscle, such as lipoma, liposarcoma, and rhabdomyosarcoma, should be excluded [5,6]. In addition, because the axilla contains abundant neurovascular tissue, blood vessel diseases, such as vascular malformations and pseudoaneurysms, and masses originating from nerves, including neurofibroma, schwannoma, and malignant peripheral nerve sheath tumors, also need to be excluded [2,7]. Radiological examinations, such as mammography, sonography, CT, and MRI can be helpful in the differential diagnosis process, and confirmation can be obtained through pathological biopsy.
The breast tissue arises at the bilateral ectoderm ridge, which is ranges from the axilla to inguinal area, known as the “milk line,” and soon disappears after formation except for the small part that remains in the pectoral region. Among the various diseases that can occur in the axilla, ectopic breast tissue occurs when the regression of this primitive mammary tissue fails at a location other than the pectoral breast [2,8]. Ectopic breast tissue can be accompanied by a nipple and areola which has been reported in diverse locations, including the face, thigh, abdominal wall, perineum, and vulva [9,10]. Hormonal influences, as well as physiological and pathological changes such as fibrocystic disease and carcinoma, may occur in ectopic breast tissue through the same mechanisms as in normal breast tissue [11]. The prevalence of ectopic breast tissue is reported to be 0.2% to 6%, and it is known that the prevalence is relatively high in Asian populations compared to in Caucasian populations [1]. Although approximately 60% of all cases have been reported to occur in the axilla, ectopic breast tissue in men is rare, accounting for 5.3% of total cases [12].
Asymptomatic ectopic breast tissues do not require additional treatment and can be monitored for malignant changes [13]. The treatment of choice for ectopic breast tissue is preventive total mass excision, which is recommended if there are functional symptoms or cosmetic discomfort [14]. Liposuction may be a treatment option and may be performed alone or as an auxiliary method of surgical excision [14].
In our case, surgical excision and pathological biopsy were performed after comprehensively considering the rapid increase in the size of the mass in the previous month, the discomfort in the patient’s daily life due to the giant axillary mass, hyperpigmentation of the axillary skin, and preoperative CT findings that could not exclude soft tissue sarcoma.
We report a clinical case of total excision and pathological evaluation of a rare giant axillary mass classified as ectopic breast tissue in a male patient and suggest the need to reconsider the possibility and differential diagnosis of various diseases that have rarely been reported in male patients and the need for further research on such conditions.