INTRODUCTION
Neoadjuvant chemotherapy (NAC) is increasingly being used for the benefits of tumor downstaging to facilitate breast-conservation therapy, to assess in vivo response to therapy, and to potentially downstage axillary lymph nodes (ALNs) [1-3]. NAC is also widely used in patients with early stage breast cancer. However, not all patients with breast cancer benefit from NAC. There may be identifiable subgroups that benefit more from this treatment than do other subgroups [4,5]. Therefore, numerous surrogate endpoints have been investigated in the setting of NAC. Rates of pathologic complete response (pCR) range from 16% to 20% according to the histologic subtypes of tumor and treatment modalities. Achievement of pCR has been correlated with better disease-free survival (DFS) and overall survival (OS) [6-8].
Recent studies have used gene expression profiling to classify breast cancers into distinct molecular subgroups and have suggested that this categorization could be used to predict prognosis. In patients treated with NAC, molecular subtype according to gene expression profiling could also effectively identify patients who are likely to achieve pCR [9-11]. The purpose of our study was to evaluate prognosis according to molecular subtype and clinicopathologic factors in patients with locally advanced breast cancer treated by NAC.
METHODS
We retrospectively analyzed the medical records of 135 patients with breast cancer who underwent NAC followed by surgery between January 2005 and January 2010. Exclusion criteria were distant metastases at diagnosis or inadequate follow up. In total, 91 patients were enrolled in this study.
All patients underwent core needle biopsy before surgery and surgical resection for breast cancer with sentinel lymph node biopsy (SLNB) and/or ALN dissection after NAC. The anthracycline- and taxane-based NAC regimens were chosen based on ALN involvement.
After completion of NAC, the patients underwent dynamic contrast-enhanced breast magnetic resonance imaging for measuring tumor size.
Patients were classified into the previously suggested immunohistochemistry (IHC)-based molecular subgroups as follows: luminal A (estrogen receptor [ER]-positive or progesterone [PR]-positive/human epidermal growth factor receptor 2 [HER2]-negative), luminal B (ER-positive or PR-positive/HER2-positive), HER2 enriched (ER-negative and PR-negative/HER2-positive), and triple negative (ER-negative, PR-negative, and HER2-negative). ER, PR, and HER2 were evaluated using standard avidin-biotin complex immunohistochemical staining methods. The ER and PR status was assessed using the Allred score, which was expressed as the sum of the proportion score and the intensity score of positively stained tumor cells. Tumors with an Allred score of at least 3 were regarded as positive. The intensity of HER2 staining was scored as 0, 1+, 2+, or 3+. Tumors with a 3+ score were classified as HER2 positive, and tumors with a 0 or 1+ score were classified as HER2-negative. In tumors with a 2+ score, gene amplification using silver in situ hybridization was used to identify HER2 status.
After completion of NAC, the size and extent of residual cancer were measured. The pCR was defined as the complete disappearance of invasive carcinoma in the breast and axilla. Residual ductal carcinoma in situ was included in the pCR category. All specimens were reviewed by an experienced pathologist.
Intraoperative subcutaneous injection of diluted indigo-carmine dye in the subareolar area was performed in the same fashion according to the surgeon’s standard SLNB practice.
Wilcoxon signed-rank tests, Kruskal-Wallis tests, Mann-Whitney U-tests, Fisher’s exact tests, logistic regression, Spearman’s correlations, and binary logistic regression analyses were used as appropriate. All variables were subjected to univariate analyses, and then the variables that were associated (p≤0.1) were analyzed in a stepwise multivariate logistic regression model. Analyses were performed using the SPSS version 19.0 statistical software package (IBM Corp., Armonk, USA), with p<0.05 considered significant.
RESULTS
This retrospective study included 91 female patients with a median age of 46 (27–78) years. Their mean body mass index was 24.0 kg/m2. A total of 59 patients (64.8%) underwent mastectomy, 89 patients (97.8%) underwent ALN dissection, 85 patients (93.4%) had invasive ductal or lobular carcinoma, and 43 patients (47.3%) were at clinical stage T4. The pCR rate was 8.8% (8 patients); however, 31 patients (34.1%) had stage ypN0 disease. The number of patients with positive ER, PR, and HER2 status were 44 (48.4%), 37 (40.7%) and 35 (38.5%), respectively. Lymphovascular invasion (LVI) was observed in 36 patients (40.0%), 87 patients (95.6%) were treated with taxane based NAC, 75 patients (82.4%) underwent radiation therapy, 43 patients (47.3%) underwent hormonal therapy, and 16 patients (17.6%) underwent trastuzumab therapy (Table 1).
Thirty five patients had luminal A, 13 had luminal B, 22 had HER2 enriched, and 21 had triple negative (TN) breast cancer. Most of the patients were in clinical stage 3, and 36 patients (39.6%) were in clinical stage 3B (Table 2). Patients with luminal A cancer tended to be less than 50 years of age (p<0.001) and had a middle histologic grade (p=0.04). Patients with luminal B, HER2-positive, and TN cancer tended to be more than 50 years of age (p<0.001) and had a high histologic grade (p=0.04). There was no statistically significant difference in laterality (p=0.612), clinical T stage (p=0.974), surgical method (p=0.253), ypT stage (p=0.591), ypN stage (p=0.15), or LVI (p=0.067) according to molecular subtype (Table 3). In this study, 6 patients showed pCR and patients with a high histologic grade tended to show pCR, but there was no statistical relation between pCR and other clinical factors such as; age, clinical stage, molecular subtype, LVI, recurrence, or death (Table 4).
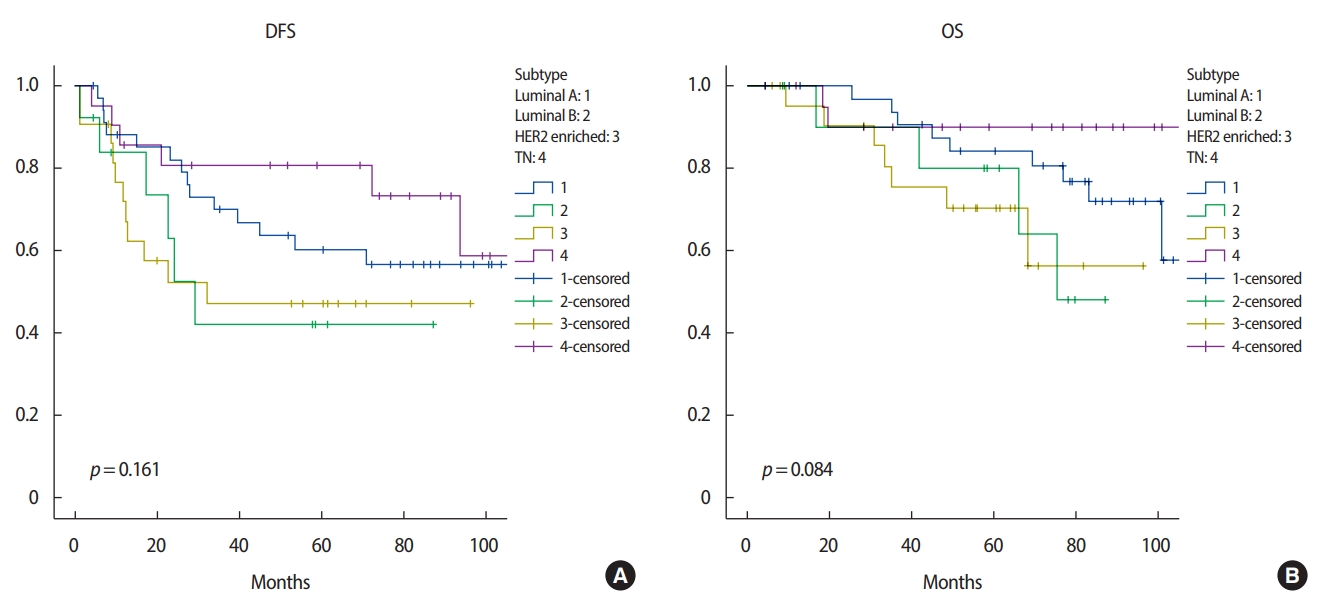
There were significant differences in 5-year DFS according to ypN stage (ypN0 vs. ypN1–3; p=0.019) and LVI (no vs. yes; p=0.003) in the univariate analysis. In the multivariate analysis, LVI was a significant factor in 5-year DFS (odds ratio 2.145, 95% confidence interval 1.064–4.324, p=0.033) (Table 5). There was a significant difference in 5-year OS according to ypN stage (ypN0 vs. ypN1–3; p= 0.005) and LVI (no vs. yes; p= 0.006) (Table 6). Molecular subtype was not a significant factor in 5-year DFS or 5-year OS, for which histologic grade had no meaning. We found no significant difference between molecular subtypes in 5-year DFS (p= 0.161) (Figure 1A) or 5-year OS (p= 0.084) (Figure 1B).
DISCUSSION
Few studies have reported differences in tumor cellularity and treatment response patterns of four breast cancer molecular subtypes. Intrinsic differences between the histopathologic characteristics of these subtypes were confirmed in our study. Molecular classification based on gene expression profiling has led to a better understanding of the biological phenotypes of breast cancer [9,12]. This is useful in predicting chemo sensitivity as well as prognosis. However, the technical complexity and high costs of this procedure have limited its clinical application. Thus, a combination of immunohistochemical profiles (ER, PR, and HER2) has been investigated as a substitute for the molecular subtypes using gene-expression profiles, although these do not exactly correspond. In this study, we found that the IHC-based molecular subtypes effectively stratified breast cancer for predicting the likelihood of pCR to NAC.
Among the four IHC-based molecular subtypes, patients with the luminal A type (that is, hormone receptor-positive) breast cancer were less likely to achieve pCR [9]. A recent randomized phase II trial showed that neoadjuvant endocrine therapy is effective in ER-positive tumors, producing similar pCR rates as NAC, and better tolerability than NAC [13]. Therefore, neoadjuvant endocrine therapy may be a promising alternative strategy in luminal A breast cancer. In patients with HER2-positive cancer, recent phase III studies have shown that pCR rates were significantly improved with the addition of trastuzumab to conventional chemotherapy [14]. We also found that in patients with HER2-positive tumors, the pCR rate for the trastuzumab-treated group, was nearly twice that for the non-trastuzumab-treated group [15,16]. The differences between the two groups were statistically significant after adjustment for confounding factors. Taking these results together, we believe that trastuzumab should be incorporated into NAC for HER2-positive breast cancer. In patients with the TN subtype, because the prognosis of those who failed to achieve pCR is very poor, achieving the highest possible pCR may be particularly important. Therefore, increasing the efficacy of NAC by adding new drugs, such as platinum or poly ADP ribose polymerase inhibitors, might be required to improve the survival of this subgroup [17].
Several studies have reported the association of ALN status and the pathologic primary tumor response to NAC. In previous studies, the response rate of primary breast tumors was correlated with that of the lymph nodes, which were well correlated with DFS [18-20]. However, tumor size, histological grade, and HER2 status were not correlated with patient outcome. In the study of Rouzier et al. [21], high histologic grade and a greater than 50% response to chemotherapy were associated with negative conversion of ALN after NAC. Our results also showed that a high histologic grade and a better response of the primary breast tumor were associated with negative conversion of ALN (Table 6).
There are several limitations in our study. First, this was a retrospective study from a single center and the total number of patients was relatively small. A larger multicenter study with more patients is needed to validate our results. Second, we did not evaluate the recurrence of ALN after surgery because of the relatively short duration of follow-up. A follow-up study of ALN recurrence is needed for better understanding of cancer biology after NAC.
LVI was associated with DFS in patients with locally advanced breast cancer treated by NAC and surgery. However, molecular subtype had no effect on 5-year DFS or OS.