INTRODUCTION
Cowden syndrome (CS), or multiple hamartoma syndrome, is a rare hereditary autosomal dominant disorder caused by a mutation in the phosphatase and tensin homolog (PTEN) gene on chromosome 10 with characteristic hamartoma of multiple organs [1-3]. PTEN is a tumor suppressor gene that controls phosphate, which mediates proliferation, progression, and apoptosis in the cell proliferation [4]. The incidence of CS is 1/200,000 individuals, and this syndrome is very difficult to diagnose clinically. The clinical features of CS are variable, presenting primarily as mucocutaneous lesions (99%). A mucocutaneous lesion, such as trichilemmoma of the face or keratosis of the extremities, is an important diagnostic marker for CS [5,6]. CS has been reported to increase the incidence of benign and malignant neoplasms in the breast, thyroid, and gastrointestinal tract [1-3,7]. The risk of developing breast cancer is up to 10 times higher in individuals with CS than in the general population throughout an entire life time [8]. The risk of developing breast cancer is up to 25%–50% times higher in individuals with CS than in the general population. Herein, we present a case of CS with synchronous bilateral breast cancer.
CASE REPORT
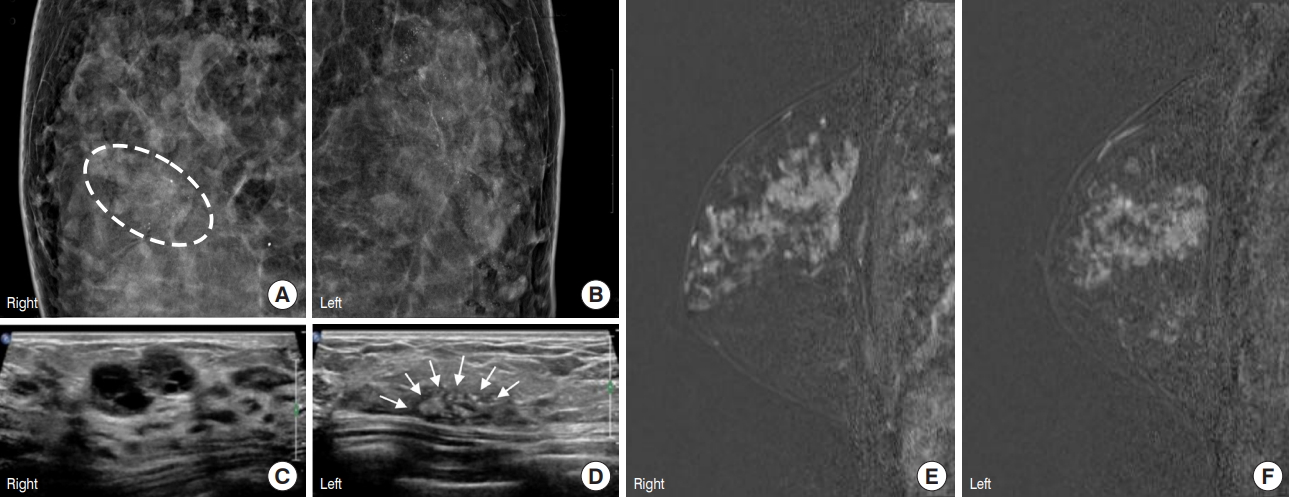
A 27-year-old woman presented with ill-defined firm masses in both breasts without palpable axillary nodes. She had no family history of breast carcinoma. However, she was previously diagnosed with CS at the age of 16 years. She had macrocephaly and multiple polyps in the oral cavity, pharynx, and gastrointestinal tract, as well as benign breast tumors and a nodular goiter of the thyroid gland when diagnosed. She underwent a right lobectomy of the thyroid gland and both breast masses were excised at the age of 18 years. Histologically, the right thyroid mass revealed follicular adenoma with atypia. The pathologic analysis of the bilateral breast masses in both breasts indicated a phyllodes tumor and tubular adenoma. She was followed up with breast ultrasonography every 1–2 years; an imaging study showed multiple Breast Imaging-Reporting and Data System (BI-RADS) category 3 masses in both breasts that had not changed. Nevertheless, at the age of 27 years, she again presented with masses in both breasts. Physical examination revealed multiple 2.5 cm-sized ill-defined and firm masses in the upper outer quadrant of both breasts without palpable axillary lymph nodes. Mammography and breast ultrasonography were performed, and they showed that segmentally distributed pleomorphic microcalcifications in the left upper outer quadrants (Figure 1A and 1B) and multiple hypoechoic mass lesions in both breasts (Figure 1C and 1D). The radiologist concluded suspicious lesions of BI-RADS category 4a in both breasts. The patient then underwent ultrasonography-guided core biopsies of the suspicious lesions in both breasts, the pathologic report revealed ductal carcinoma in situ (DCIS) of both breasts. To decide on surgery, we performed breast magnetic resonance imaging, which revealed diffusely distributed, heterogenous, and nodular non-mass enhancement of approximately a 9.0-cm sized area in both breast upper outer quadrants (Figure 1E and 1F). According to this finding, we performed the bilateral skin-sparing mastectomy with immediate breast reconstruction. Breast reconstruction was performed using implants by plastic surgeons.
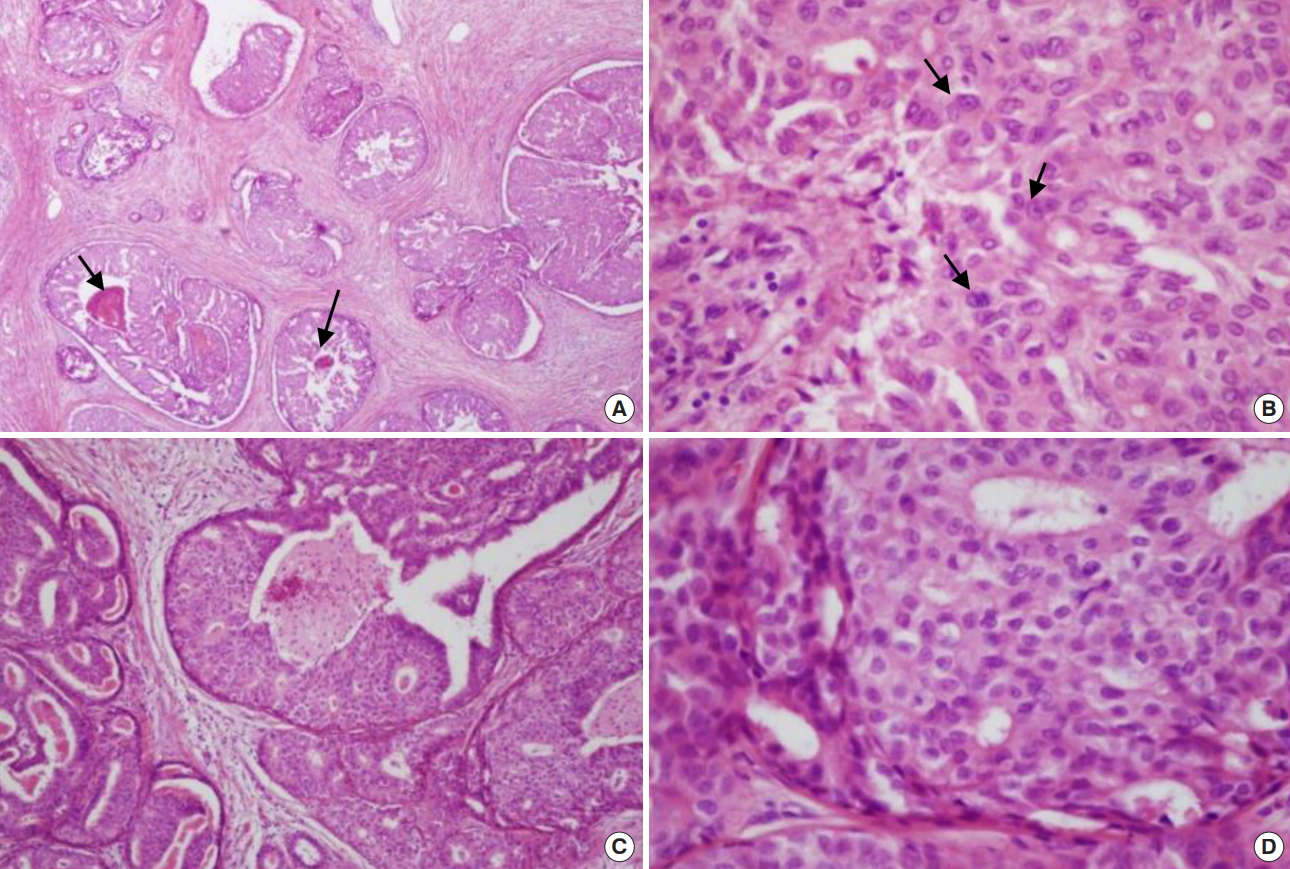
The final pathologic report showed that macroscopically, bilateral breast tissues bilaterally showed ill-demarcated, pale tan, and diffuse firm and nodular lesions without definite masses. Microscopically, the tumor from the right breast consisted of DCIS of intermediate grade that was predominantly cribriform type (Figure 2A and 2B). Different from the tumor in the right breast, the tumor in the left breast revealed DCIS of high-grade with various types, such as papillary, cribriform, solid, and comedo-type (Figure 2C and 2D).
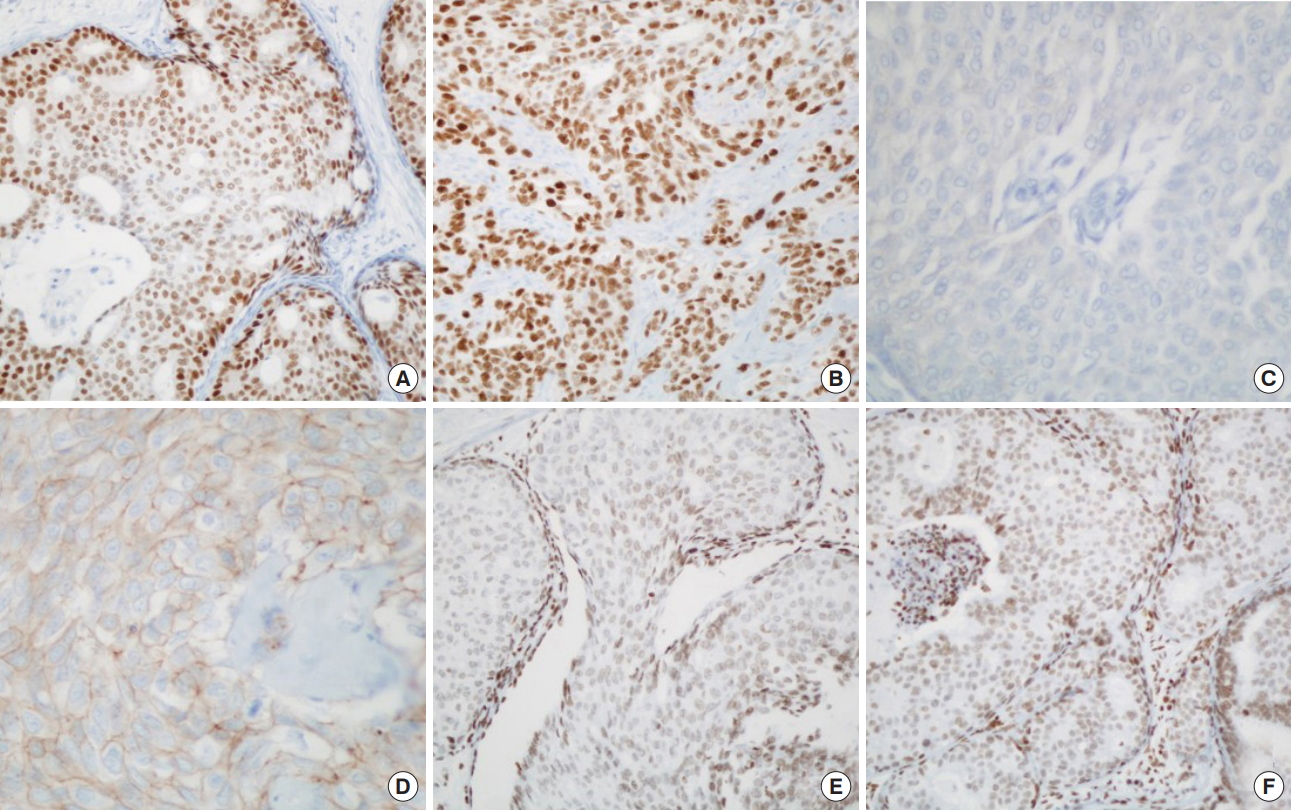
Immunohistochemistry (IHC) of estrogen receptor showed positive in both breast tumors (Figure 3A and 3B). IHC of human epidermal growth factor receptor 2 (HER2) revealed negativity in the right breast tumor (Figure 3C). However, in the left breast, IHC of HER2 showed positive membranous staining (Figure 3D). IHC of PTEN revealed positive nuclear staining in both breast masses (Figure 3E and 3F).
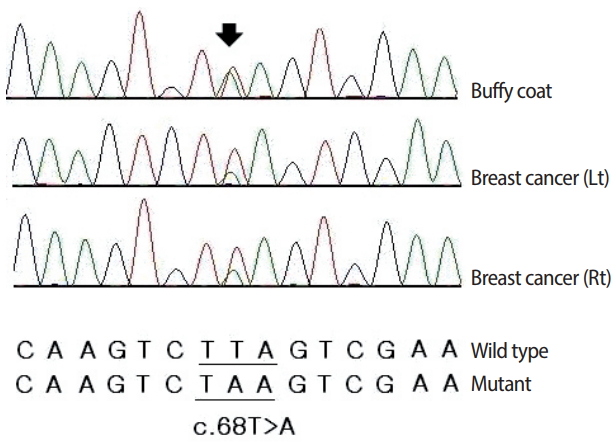
The mutational analysis of PTEN was performed by using polymerase chain reaction (PCR) amplification and direct sequencing of all nine exons of the gene, including the splicing regions. Blood and cancer tissue samples were obtained from Keimyung University Dongsan Hospital Biobank, Korea. Informed consent was obtained, and the protocol was approved by the Institutional Review Board of Dongsan Medical Center (DSMC 2014-10-051). Genomic DNA was extracted, and PCR was performed using Smart Tag Pre-mix (Solgent Co., Daegu, Korea). PCR primers for PTEN were designed using Primer3 (http://frodo.wi.mit.edu/primer3) (Table 1). Products were purified and bidirectionally sequenced using a BigDye Terminator v3.1 Cycle Sequencing kit (Applied Biosystems, Foster City, USA) on an ABI 3730XL DNA analyzer (Applied Biosystems). For all sequencing results, traces were reviewed by the Sequencherv5.2.4 software (http://genecodes.com/). DNA sequencing analysis detected the heterozygous transversion c.68T>A in exon 1 from both breast cancer tissues and peripheral blood (Figure 4). This was a pathogenic nonsense variant resulting in the substitution of a residue of leucine on codon 23 with a stop codon (leu23Ter).
The patient did not require additional treatment for bilateral DCIS and no further routine breast examinations were performed because of the bilateral mastectomy. However, further imaging studies are necessary for early detection of secondary malignancies, e.g., uterine or renal malignancy during the follow up period.
DISCUSSION
CS, also known as multiple hamartoma syndrome, is an autosomal dominant disorder caused by a germline inactivating mutation of the PTEN gene located on chromosome 10q23.31-3 [1-3]. The clinical diagnostic criteria for multiple hamartoma syndrome have been established and revised; major and minor criteria are listed in Table 2 [9]. CS is suspected if a person meets three major criteria which must include either macrocephaly, Lhermitte-Duclos disease [10], or gastrointestinal hamartomas, or two major and three minor criteria. In families where one individual meets the clinical diagnostic criteria of CS or has a PTEN mutation, CS is suspected if a person has either any two major criteria with or without minor criteria, one major and two minor criteria, or three minor criteria. With the identification of PTEN involvement in CS, the incidence of the syndrome has increased to 1/200,000 individuals.
Herein, we reported a woman with CS presenting with thyroid follicular adenoma, multiple intestinal hyperplastic polyps, and synchronous bilateral breast DCIS over 10 years. The syndrome was diagnosed when the patient was 16 years old and she underwent bilateral mastectomy when she was 27 years old. It is critical to note that malignant transformation can occur in young patients with CS, in the form of bilateral and synchronous lesions of the breast. As was the case for this patient, adequate follow-up examinations for the organs known to undergo malignant transformation in CS should be performed in patients with early-onset. When benign lesions are observed, the possibility of transformation into malignant tumors should be acknowledged, and follow-up examinations should be performed consistently over the patient’s life time [11,12]. We advise that clinical management of all patients with CS should consist of an early multidisciplinary surveillance program initiating from the time of diagnosis.