INTRODUCTION
Neoadjuvant chemotherapy increases the possibility of breast conserving surgery (BCS) for locally advanced breast cancer [1-4]. In prospective study in Korea, the conversion rate from mastectomy to BCS was 40.5% in triple negative breast cancer (TNBC) [4]. However, patients who required neoadjuvant chemotherapy had an anxiety or depression disorder because of long periods of treatment before surgery, and side effects such as alopecia, nausea, and diarrhea [5]. Although neoadjuvant chemotherapy should be considered as the first option for advanced TNBC, surgery might be considered in stage II to IIIA if the patient strongly insists that surgery should be performed first. However, TNBC has a higher locoregional recurrence (LRR) and visceral metastases than other subtypes of breast cancer [6-8]. Therefore, there is a concern that mastectomy should be considered in patients with TNBC. Several studies have investigated whether BCS achieved better outcomes than mastectomy, but the results are controversial [9-12]. We compared the outcomes of BCS and mastectomy in patients with stage II-IIIA TNBC. Furthermore, we assessed prognostic factors for recurrence or metastasis.
METHODS
Patients
The patients were diagnosed with primary TNBC and treated at Pusan National University Hospital and Pusan National University Yangsan Hospital from 2010 to 2014. The patients were treated with surgery and adjuvant chemotherapy, or radiation therapy. Patients with ductal carcinoma in situ, stage I, IIIB, and IIIC, recurrent breast cancer, metastases at diagnosis, or neoadjuvant chemotherapy were excluded.
Age at diagnosis was used to analyze the survival period. We assessed the type of surgery, histology, tumor size, lymph node status, tumor grade, type of chemotherapy, and radiation therapy. In the BCS group, an intraoperative frozen biopsy was obtained from the remnant breast tissue, and additional breast tissue was resected when the frozen biopsy results were positive. The surgical margin was assessed as negative when the final pathologic report confirmed that “no tumor was present”.
Hormone receptor status was graded using Allred scoring and scores of 3-8 were considered positive. TNBC included tumors that were negative for hormone receptors and human epidermal growth factor receptor 2 (HER2). The cancers were staged according to the breast cancer guidelines of the 8th American Joint Committee on Cancer (AJCC).
We monitored patient status every three to six months for the first five years after primary therapy and annually thereafter. The date and cause of death were obtained from the medical records of the deceased patients. LRR was defined as recurrence in the ipsilateral breast, chest wall or axillary, supraclavicular, infraclavicular, or internal mammary nodes. Metastasis in any other organ was considered a distant metastasis. LRR-free survival (LRRFS), disease-free survival (DFS), and overall survival (OS) were measured from the date of surgery to the date of LRR, the time of recurrence or metastasis, and either death or the date the patient last visited the outpatient clinic, respectively.
This study was approved by the Institutional Review Board of Pusan National University, Korea (IRB No. 04-2020-011).
Statistical analyses
The demographics and tumor characteristics were compared between the BCS and mastectomy groups using Chi-squared tests. If a variable with a significant difference between the two groups was a factor that affected LRR or metastasis, we performed an adjusted multivariate logistic regression analysis. The Kaplan-Meier method was used for the LRRFS, DFS, and OS comparisons by the log-rank test, and p< 0.050 was considered significant. The Cox proportional hazards model was used to select significant covariates. The data were analyzed using SPSS version 21 (SPSS Inc., Chicago, USA).
RESULTS
Altogether, 172 patients diagnosed with stage II-IIIA TNBC from 2010 to 2014 were included in this study. The median age of the patients was 51 years (range, 22-82 years). One hundred and one (58.7%) patients underwent BCS, while 71 (41.3%) underwent mastectomy. The patient and tumor characteristics between the two groups are summarized in Table 1. Compared to the BCS group, the mastectomy group had a higher tumor stage (T stage), more stage IIIA patients, and a lower proportion of Ki-67. In the BCS group, 97.0% of the patients received radiotherapy compared to 62.0% of the patients in the mastectomy group (p< 0.001). Of the three patients (3.0%) in the BCS group who did not receive adjuvant radiotherapy, two patients refused radiotherapy, and one developed a LRR before the planned radiotherapy. One hundred (99.0%) patients in the BCS group received chemotherapy compared to 64 (90.1%) patients in the mastectomy group (p= 0.007).
Overall, 31 patients (18.0%) had a LRR or distant metastasis with a median follow-up period of 71 months (range, 6-113 months). LRR occurred in 18 patients: eleven in the BCS group and seven in the mastectomy group. Distant metastases was seen in 22 patients: 12 in the BCS group and 10 in the mastectomy group.
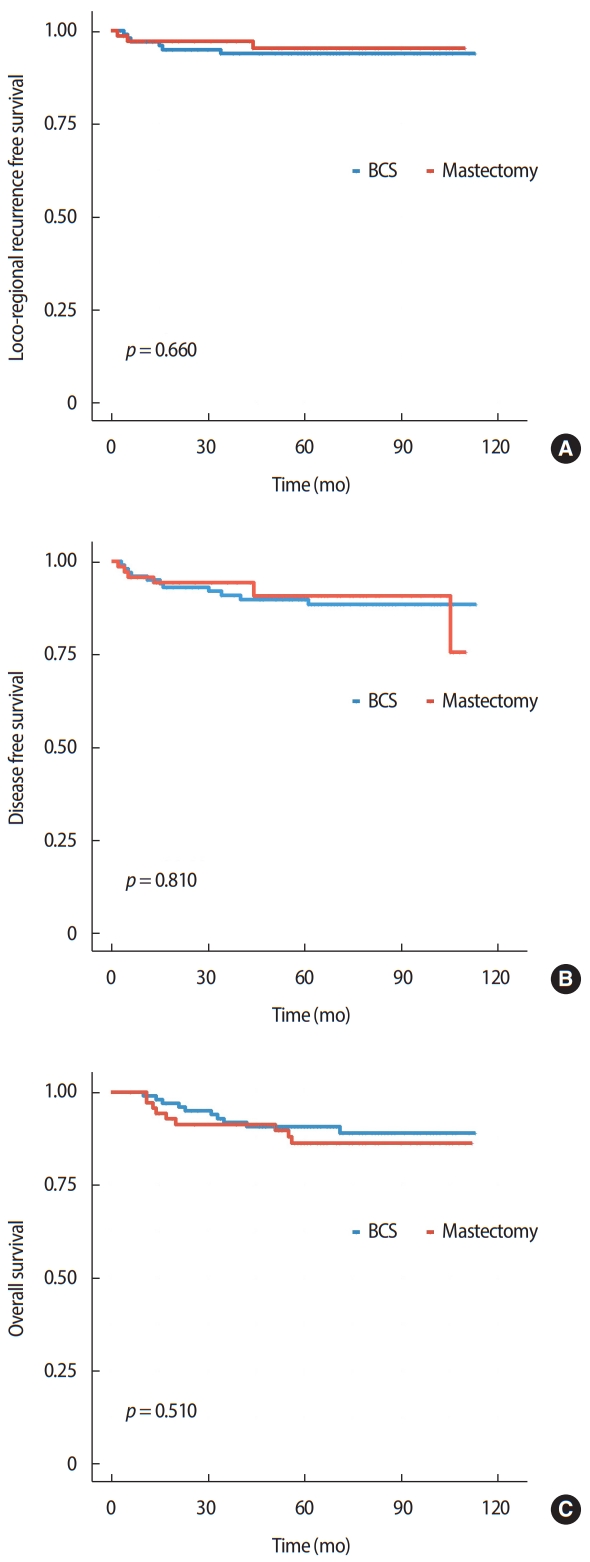
The 5-year LRR-free, disease-free, and overall survival rates of the BCS versus mastectomy groups were 93.8% vs. 95.3%, 89.8% vs. 90.7%, and 90.8% vs. 86.3%, respectively, but the differences were not statistically significant. Figure 1 shows the Kaplan-Meier curves for LRRFS, DFS, and OS according to the differences in surgical methods.
The absence of lymphovascular invasion (LVI) was significantly associated with superior DFS on multivariate analysis (p = 0.047). As shown in Table 2, advanced stage was significantly associated with OS on multivariate analysis, but there were no significant factors affecting LRRFS in multivariate analysis.
The tumor stage (T stage) could be a confounding variable because the pT stage was higher in the mastectomy group than in the BCS group. Therefore, we performed an adjusted multivariate logistic regression analysis according to the pT stage. However, as shown in Table 3, whether the T stage was classified as T1, T2, and T3, or classified as group T1 and T2 combined, and group T3, the difference in surgical method did not affect LRR or metastasis.
DISCUSSION
Mastectomy is often preferred over BCS because of the aggressive features of TNBC. However, some studies have demonstrated that BCS has better outcomes than mastectomy in the early stages of TNBC [12-15]. Therefore, this study excluded stage I TNBC when comparing the results of BCS and mastectomy. In addition, we excluded patients who received neoadjuvant chemotherapy to obtain accurate pathological results. If patients are diagnosed with stage II to IIIA breast cancer after surgery following neoadjuvant chemotherapy, it would be difficult to accurately compare them to the patient groups in this study because of the debulking effect of neoadjuvant chemotherapy. When breast cancer has penetrated the skin, or there are multiple lymph node metastases on preoperative examination, neoadjuvant chemotherapy should be considered first [16]. Therefore, patients with stage IIIB and IIIC breast cancer were excluded to minimize bias from these selections. As mentioned in the results of this study, BCS was not inferior to mastectomy, and the results were similar to those of previous studies [17-19]. However, the limitations of the study by Chen et al. [18] were inadequate follow-up duration and the lack of available information on adjuvant chemotherapy or neoadjuvant chemotherapy. A meta-analysis by Wang et al. [19], indicated that BCS showed an improvement in LRR compared to mastectomy, but this study did not perform stage-related comparisons. In the current study, the median age of the patients was 51 years, which was consistent with other research reports showed that Korean women in their mid-forties had a high breast cancer incidence rate, unlike the rate in Western countries [20,21]. Therefore, BCS is performed more frequently than mastectomies. The BCS methods included a quadrantectomy with a local flap, latissimus dorsi musculocutaneous flap (LDMCF) with or without saline bag insertion, and reduction mammoplasty. We performed quadrantectomy to ensure sufficient margins in the BCS group. As mentioned in the methods section, when the intraoperative frozen biopsy margin was positive, breast tissue was resected until the biopsy was confirmed as negative. However, there were two cases in which atypical cells were identified in the final pathological results, and these patients were treated with radiotherapy. Mastectomy included total mastectomy, nipple-sparing mastectomy, and skin-sparing mastectomy with or without axillary lymph node dissection. All except three of the patients in the BCS group received adjuvant radiotherapy, and 6.2% of the patients in this study had LRR at five years after BCS. Considering that 4.7% of the patients in the mastectomy group had LRR after five years, BCS with radiotherapy followed by adjuvant chemotherapy achieved good results in patients with stage II-IIIA TNBC. Although radiotherapy was not completely excluded in the mastectomy group, adjuvant radiotherapy could significantly reduce the risk of LRR in TNBC [22]. Further, except for one patient, adjuvant chemotherapy was performed more often in the BCS group (Table 1). In the mastectomy group, out of seven patients who did not received adjuvant chemotherapy, there was one patient with LRR and one with liver metastasis. A 55-year-old patient refused chemotherapy and radiotherapy after mastectomy because of a psychiatric problem, and a 69-year-old patient refused both treatments after mastectomy. In this study, multivariate analyses showed that chemotherapy was not a significant prognostic factor. In addition, the presence of LVI was related to poor prognosis, and this result has further been reported in other studies [14,17,23,24]. Therefore, more intensive treatment should be considered for TNBC patients with LVI.
This study had several limitations due to its retrospective design. Radiotherapy, chemotherapy, the value of Ki-67, and pT stage were different between the two groups, and selection biases were not completely resolved. In particular, the higher the pT stage, the more often mastectomy was performed compared to BCS (Table 1). Since the pT stage was a confounding variable that could affect outcomes such as LRR, we conducted an adjusted multivariate logistic regression analysis. As a result, though we included the pT stage in the model and adjusted for the pT stage, the difference in surgery type did not affect LRR or metastasis (Table 3).
Despite these limitations, the follow-up period was relatively long. As in other studies, there was no significant difference in the outcomes between BCS and mastectomy in the advanced stages [10,17]. Although neoadjuvant chemotherapy is considered as the first treatment option for advanced stage triple negative breast cancer, BCS could be selected if patients want to undergo surgery first even in the advanced stage.
In conclusion, BCS could be considered in patients with advanced TNBC patients because it has been shown that the outcomes of BCS are not inferior to those of mastectomy.