INTRODUCTION
Recent advances in treatment modalities of breast cancer have led to significant improvement in patient outcomes. The quality of life for breast cancer survivors has become a more important issue. Patients who undergo mastectomy can suffer from impairment of body image, loss of sexual function, or emotional disturbances, which may negatively impact quality of life. Many studies have established that breast reconstruction performed at the time of mastectomy, termed IBR, can reduce psychosocial problems and improve quality of life. The improvement in both implant and autologous techniques, thus, providing better aesthetic results, has led to a rapid expansion of IBR over the past 2 decades [1-4]. Immediate reconstruction has been shown to be both feasible and oncological safe without any evidence of increased mortality when compared with delayed reconstruction or mastectomy alone. However, relatively small series of patients with advanced stage cancer were involved in most studies of the relationship between breast reconstruction and survival outcomes, whereas large cohorts with early stage breast cancer were well evaluated [5-9]. Several reports have regarded patients with LABC as unfavorable candidates for IBR because of high recurrence rate and concerns about further exacerbated mortality caused by disturbance in detecting local relapse lesions and delays in postoperative therapy [10-16]. As current multi-modality treatments including chemotherapy, targeted therapy and post-mastectomy radiotherapy (PMRT) are essential to improve survival outcome in LABC, a possible delay in the delivery of adjuvant therapy due to IBR has become a matter of concern. This in turn may negatively affect recurrence and survival rates. There are some studies that demonstrated no statistically significant differences in survival outcomes between those underwent IBR vs. mastectomy alone. According to the study using the Surveillance, Epidemiology, and End Results (SEER) data, there are comparable survival outcomes in LABC patients who received immediate breast reconstruction or mastectomy alone followed by PMRT. The purpose of this study was to evaluate and compare clinical characteristics and survival outcomes between patients with LABC who received mastectomy alone or IBR in a single institution.
METHODS
We obtained data from the Seoul National University Hospital Database. The analysis included cases diagnosed with clinical stage III or pathological stage III breast cancer and underwent curative operation between January 2004 and December 2015. The patients who underwent total mastectomy, radical mastectomy, modified radical mastectomy, skin sparing mastectomy, or nipple-areolar-complex sparing mastectomy were included. We identified 77 and 171 patients with or without IBR, respectively. All the patients were over 18 years old when they were diagnosed. All patients with a follow-up length less than 12 months, or inadequate amount of data were excluded. The following data collected: BMI, age-at-diagnosis, histologic type and grade, hormone receptor status, human epidermal growth factor receptor-2 (HER2) status, clinical or pathologic stage, modality of adjuvant treatment, endocrine therapy, monoclonal antibody therapy, time to adjuvant chemotherapy, fertility preservation, type of reconstruction and DFS. The breast cancer was pathologically staged according to 7th AJCC criteria. We reviewed the electronic medical records of the patients to identify the occurrence of loco-regional recurrence or distant metastasis and type of reconstructive materials. This study was conducted with the approval of the Institutional Review Board of Seoul National University Hospital (IRB No. H-1812-066-993).
At present, many patients have already been terminated, died, or have been transferred to other hospitals. Patients who are still being treated at our hospital have a follow-up period of more than 6 months, so it is not practical to obtain individual consent for a large number of patients. Since this study is a retrospective cohort study through retrospective medical records review, there is no additional harm to patients except the exposure of personal medical records information. In this respect, we were granted a waiver of consent.
We defined loco-regional recurrence as the recurrence on remnant skin, ipsilateral chest wall or ipsilateral regional lymph nodes. Distant recurrence was defined as recurrence at any distant organ or lymph nodes except ipsilateral axilla and cervical area. DFS was defined as the length of time after surgery for primary breast cancer to the earliest report of any loco-regional or distant recurrence
RESULTS
Patients and tumor characteristics
Among 248 patients who were enrolled in this study, 77 women underwent breast reconstruction at the time of mastectomy and the other 171 had mastectomy performed without reconstruction. The clinical and pathologic information of the two groups are listed in Table 1. Median follow-up time was 49 months and the mean age of patients was 49 (range 28–84) years in this study population. The patients with IBR were significantly younger than women that received MA (43 vs. 55, p<0.001) and no patient older than 55 years underwent IBR in our cohort. BMI of the patients with IBR was lower than that of patients who had MA performed (22.2 vs. 23.4, p=0.001). The IBR group had a higher rate of being progesterone receptor-positive, but there was no difference between the two groups regarding endocrine therapy was required (Table 1).
Treatment modality
The patients in both groups were treated by neo- and adjuvant chemotherapy, endocrine therapy and/or radiotherapy in accordance with standard protocol. Briefly, 242 (97.6%) patients were treated with chemotherapy; the remaining 6 patients did not receive chemotherapy due to old age and/or poor general condition. While one-third of the patients with IBR received preoperative chemotherapy, over two-thirds of patients in the MA group were treated with preoperative chemotherapy (36.4% vs. 69.6%, p<0.001). The difference in rate of neoadjuvant chemotherapy was statistically significant between the two groups, but the response status after neoadjuvant chemotherapy was not significantly different between the two groups (Table 2). Over 90% of all patients received PMRT according to treatment guidelines. In 92 patients who were received adjuvant chemotherapy, the time to initiation of chemotherapy after surgery was not different between IBR and MA groups (34.5±26.6 vs. 31.4±10.5, p=0.470) (Table 1). When comparing the IBR group and MA group, there was no statistically significant difference in the rate of endocrine therapy with Estrogen receptor (ER) or Progesterone receptor (PR) positive (98.3% vs. 95.5%, p=0.624) (Table 1). Similarly, there was no statistically significant difference between the two groups in using Trastuzumab with HER2 positive (95.5% vs. 95.8%, p=1.000) (Table 1). The percentage of fertility preservation in the IBR group was significantly higher than that in the MA group (Table 1).
According to the modality of immediate breast reconstruction, the recurrence rate, loco-regional recurrence rate, and distant recurrence rate did not show statistically significant difference. Autologous tissue group showed longer DFS than the implant group (90.5 vs. 57.8, p=0.021) (Table 3).
Recurrence & Disease-free survival
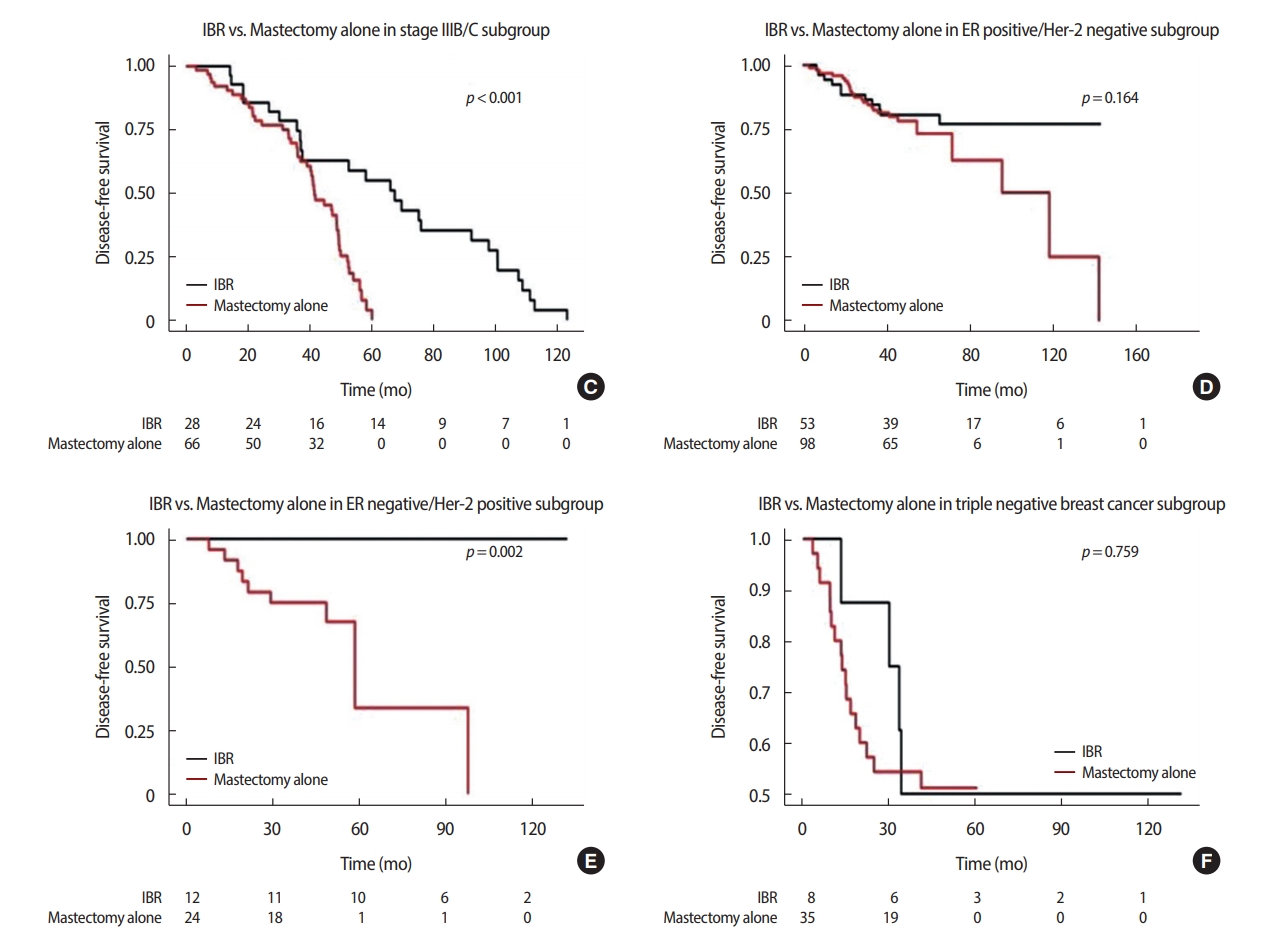
A total of 70 (28.2%) patients experienced recurrence by the follow-up date. The recurrence rate was not different between the IBR and MA group (22.1% and 31.0%, respectively, p=0.197). There were 17 (9.9%) cases of loco-regional recurrence in the patients who received MA, in contrast with two of 77 (2.6%) women who had IBR performed (p=0.079). Distant metastasis was found in 15 (19.5%) and 48 (28.1%) patients with or without IBR, respectively (p=0.200). The median DFS for women with IBR was 81.3 months, whereas for patients with MA it was 49.8 months (p<0.001) (Table 4). In a subset analysis according to stage stratification, the women who received IBR showed better DFS than those who underwent MA in both stage IIIA and, IIIB/IIIC (p<0.001). In all subtypes regarding ER and HER2 status, IBR patients were not inferior to MA patients in DFS (Figure 1).
In multivariate analysis adjusting for BMI, age-at-diagnosis, histologic grade, ER, stage, and fertility preservation, mastectomy-alone, histologic grade, and stage showed higher Hazard ratio (HR). IBR group showed significantly better DFS than MA group (HR for recurrence; 0.37, 95% CI 0.20–0.69, p=0.002) (Table 5).
DISCUSSION
When a mastectomy is mandatory due to breast cancer, recent treatment guidelines recommend that the surgeon should determine the type of operation depending on the patient’s personal preferences and the surgeon’s experience. However, it should be noted that IBR does not result in delaying appropriate surgical intervention, nor does it compromise oncological safety. In patients with advanced stage disease, there is typically more concern about the safety of IBR, but there is limited evidence to support this. Furthermore, there are conflicting results with regards to treatment delay or complication rate in LABC patients who received IBR. The present study showed that IBR in patients with stage III disease did not impair oncological outcomes, which is consistent with the findings of previous studies [17-20].
Today, with advances in multi-modality approaches that can improve the outcome of LABC [21-23], better quality of life can be achieved with IBR. This is extremely significant for survivors of breast cancer. Also, the increasing trend of using preoperative chemotherapy rather than postoperative chemotherapy for LABC has substantially reduced the concern of chemotherapy delay due to IBR [24-27]. Although the primary goal of preoperative chemotherapy is breast conservation, total mastectomy is still unavoidable when the tumor size is not reduced enough for conserving surgery, or due to the patients choice for mastectomy despite the fact that breast conservation is feasible.
There have been concerns of delay or interference with postoperative chemotherapy or post-mastectomy radiotherapy due to IBR. Our study demonstrated that there was no delay of postoperative chemotherapy in the 92 patients who eventually received it (Table 1). This is consistent with previous studies that investigated delays in adjuvant therapy due to IBR [28,29]. Frasier et al showed that recently increased use of PMRT in LABC was not associated with a decrease in IBR rate [30].
The results obtained of improved DFS in the IBR group compared with the MA group (HR 0.37, 95% CI 0.20–0.69, p=0.002) is consistent with previous studies that showed better survival outcome in patients who received reconstructions [31]. Bezuhly et al. [32] concluded that IBR is associated with decreased mortality among younger women in an analysis of US SEER data. Similarly, Hsieh [31] demonstrated that immediate TRAM flap reconstruction might be an independent predictor of favorable survival outcome. These results, including the present study, might be due to a selection bias, despite adjustment of known prognostic factors. There was no statistically significant difference in recurrence rate between the two groups that underwent autologous tissue vs. implant, but there was a statistically significant difference in DFS. A total of 24 subjects in the implant group was considered to be too small for statistical analysis (Table 3). This is an intrinsic limitation of the retrospective analysis. Also, previous reports suggested that the patients with higher socio-economic status were more likely to choose reconstruction [33-36], which can be a potentially favorable prognostic factor. Therefore, careful interpretation of these retrospective studies is needed. In any case, our results suggest that IBR did not have a negative effect on LABC patients’ long term survival.
Many possible variables were considered in the statistical analysis. The variables found to be statistically significant include BMI, age-at-diagnosis, PR status, chemotherapy-detailed, and fertility preservation. However, the difference of response status of neoadjuvant chemotherapy in the IBR group vs. MA group was not statistically significant. If ER or PR was positive, there was no statistically significant difference in endocrine therapy. Therefore, only BMI, age-at-diagnosis and fertility preservation were the non-stratification variables when comparing the two groups. We performed univariate analysis and multivariate analysis between the two groups. The results were that IBR, histologic grade and stage had a statistically significant effect on hazard ratio (Table 5).
Some weaknesses of the present study include modest length of follow-up (49 months), relatively small number of patients with low statistical power, no information on postoperative complication rate, and lack of data about morbidity or underlying medical/socio-economic status in both groups.
In conclusion, we demonstrated that IBR for LABC patients did not impair their disease-free survival outcome during an average of 49 months compared with mastectomy alone without reconstruction. In the absence of prospective study evidence, our results based on retrospective data can help surgeons choose immediate reconstruction as an option for patients with LABC.