INTRODUCTION
Human epidermal growth factor receptor 2 (HER2), a transmembrane receptor tyrosine kinase that is encoded on the long arm of chromosome 17 (17q12-21.32), is involved in tumor growth and progression. Overexpression of HER2 and gene amplification are displayed in 15% to 20% of breast cancer patients and are associated with aggressive cancer and a poor prognosis [1-4].
Trastuzumab, a representative targeted therapeutic agent for HER2-positive breast cancer, acts to arrest the cell cycle G1 phase and blocks cell proliferation with a humanized monoclonal antibody attached to the extracellular domain of the HER2 receptor. The drug, approved by the Food and Drug Administration (FDA) in 1998, has helped improve survival outcomes in both adjuvant and metastatic settings for HER2-positive breast cancer [5-8]. Clinical trials, such as NSABP B-31 and NCCTG N9831, have shown that the addition of trastuzumab in an adjuvant setting increases disease-free survival [9]. Since such HER2-targeted therapies are only indicated for HER2-positive breast cancer, identification of HER2 positivity is important [10].
HER2 positivity is generally determined by immunohistochemistry (IHC), which measures the degree of overexpression of the HER2 protein. Although IHC is inexpensive and easy to perform, HER2 positivity may often be difficult to conclusively determine due to specimen heterogeneity and reader subjectivity in the interpretation of HER2 protein expression level [11]. The HER2 in situ hybridization (ISH) method, which measures HER2/neu gene amplification, is used in cases equivocal by IHC. ISH encompasses fluorescence ISH (FISH), chromogenic ISH, silver ISH (SISH), and dual color ISH [7]. FISH, in particular, has excellent sensitivity and specificity and is used as a golden standard in this setting [10].
According to American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines, an IHC score of 3+ or gene amplification of more than six copies per nucleus by ISH qualifies as HER2 positive [6]. Although HER2 protein overexpression and HER2/neu gene amplification are closely related to each other, a debate remains on whether there is a difference in prognosis between the two for diagnosing HER2 cancer [12,13]. The aim of this study was to compare prognosis between the two methods in HER2-positive breast cancer patients.
METHODS
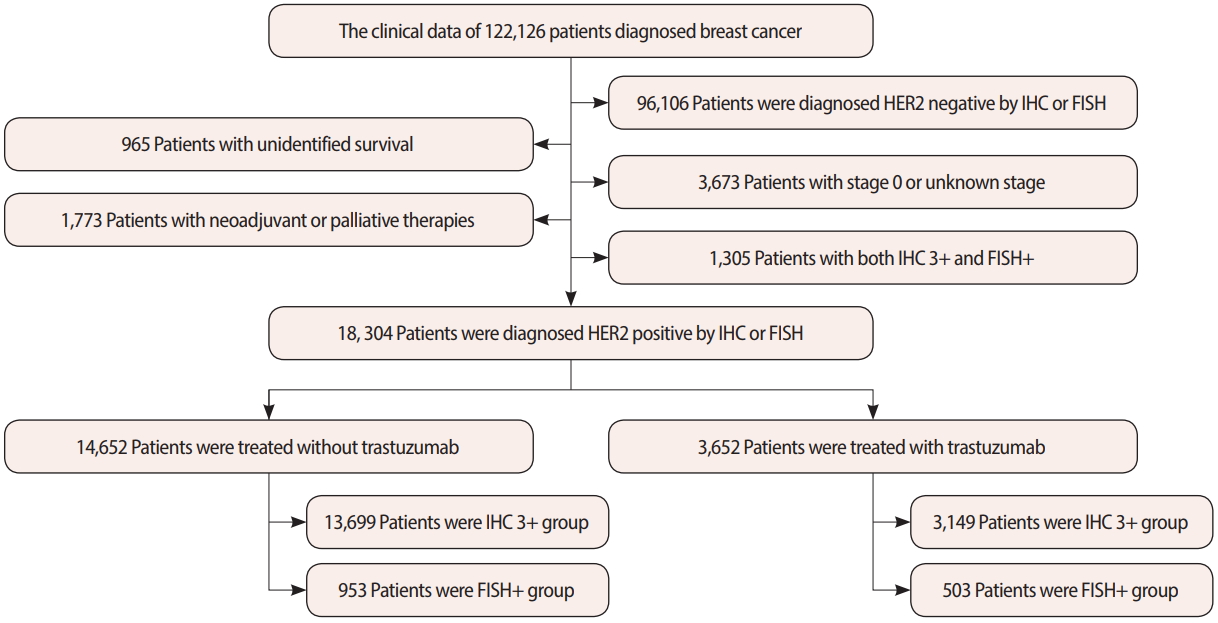
In this study, we used materials approved by the Korean Breast Cancer Society registration system (KBCR). KBCR has been registering cases submitted by breast surgeons at 110 training hospitals nationwide since 1996 and has previously been described in detail [14-17]. The cause and date of death in the documents were used in connection with the Korea Central Cancer Registration Data of the Ministry of Health and Welfare in collaboration with the Korean National Statistical Office to compile complete death statistics, which were updated through 2014. This study was approved by Daejeon St. Mary’s Hospital Institutional Review Board (IRB; No. DC16OSSI0071). The IRB approving the study did not require additional informed consent to be obtained. Of the 122,126 patients diagnosed with breast cancer from June 1983 to December 2015, 18,304 patients were included in this study after others were excluded as described in Figure 1. Of these, 14,652 patients treated without trastuzumab and 3,652 patients treated with trastuzumab were retrospectively analyzed in the 3+ group by IHC test and the HER2/neu gene amplification group by FISH. Based on the criteria for a HER2-positive diagnosis, each patient was classified as IHC 3+ and FISH+ (Figure 1). For prognostic measurements, based on the presence or absence of trastuzumab, we compared breast cancer-specific survival and overall survival between IHC 3+ and FISH+ groups, and we further analyzed factors affecting survival rate.
Immunohistochemistry
IHC follows a 4-step scoring system from 0 to 3+, which depends on the immunostaining intensity in the cell membrane of the tissue specimen, as a way to measure the amount of HER2 protein in paraffin sections of breast cancer tissue. According to ASCO/CAP guidelines, specimens are classified as 0 to absent, 1+ to faint, 2+ to weak, and 3+ to intense from more than 10% cells [18]. A score of 3+ is associated with HER2/neu gene amplification in almost all cases, and IHC alone determines HER2 positivity.
Fluorescence in situ hybridization assay
The HER2 gene is located on chromosome 17, and gene amplification is measured by displaying it. When more than six copies are shown per nucleus or when the HER2/CEP17 ratio is higher than 2.0, the sample is considered FISH+ for HER2. FISH as a predictor of response to HER2 target therapy is more sensitive and specific than IHC. Further, when IHC is equivocal (IHC 2+), FISH is used to determine HER2 positivity.
Description of the study cohort
Patient baseline clinical characteristics included age, family history, surgical method, pathological TNM stage, menopause status, diagnostic method for HER2 positive (IHC 3+ or FISH+), histologic grade, nuclear grade, and adjuvant therapies, such as chemotherapy, radiotherapy, and endocrine therapy.
Statistical analysis
Prognosis was compared using the SAS System for Windows version 9.3 (SAS Institute Inc., Cary, USA). Comparisons of baseline characteristics were performed using the Student t-test, Pearson chisquare test, or Fisher exact test. The correlation between IHC and FISH and other clinical factors was compared by logistic regression analysis, and comparisons of survival rates were performed with Kaplan-Meier methods and Cox proportional hazard models.
RESULTS
Clinicopathological characteristics
The median follow-up period was 65 months (range, 0–234 months) in the 18,304 patients. The proportion of patients who used trastuzumab was lower in IHC 3+ patients (18.7%) compared to FISH+ (34.5%) patients (p< 0.001). To consider possible prognostic differences due to trastuzumab, IHC 3+ and FISH+ patients were compared after stratification by trastuzumab treatment. Basic clinicopathological characteristics and survival were compared between patients with or without trastuzumab treatment and described as Table 1. The average and standard deviation of age was 50.21±10.38 years for IHC 3+ and 51.92±11.15 years for FISH+ patients who did not receive trastuzumab (p< 0.001), and 50.72± 9.50 years for IHC 3+ and 51.39±10.55 years for FISH+ patients who received trastuzumab (p = 0.181).
Clinicopathological factors associated with HER2 positive breast cancer according to diagnostic methods
Based on univariate logistic regression analysis in patients who did not receive trastuzumab, FISH+ was more associated with age, nuclear grade (grade 2–3), radiotherapy, and endocrine therapy, while IHC 3+ was more associated with mastectomy, axillary dissection, pathologic stage (stage III), premenopause, histologic grade (grade 2–3), negative hormonal receptor status, breast cancer-specific survival, and overall survival. In patients who received trastuzumab, FISH+ was more associated with family history, nuclear grade (grade 2), radiotherapy, and endocrine therapy, and IHC 3+ was more associated with mastectomy, axillary dissection, pathologic stage (stage III), negative hormonal receptor status, and overall survival (Table 2). In multivariate analysis, the breast cancer-specific survival and overall survival factors were analyzed separately. For breast cancer-specific survival and patients who did not receive trastuzumab, FISH+ was more associated with age, pathologic stage (stage II–IV), nuclear grade (grade 2–3), radiotherapy, and chemotherapy, and IHC 3+ was more associated with axillary dissection, histologic grade (grade 2–3), negative hormonal receptor status, endocrine therapy, and breast cancer-specific survival. In patients who received trastuzumab, FISH+ was more associated with nuclear grade (grade 2–3), and IHC 3+ was more associated with axillary dissection and negative hormonal receptor status (Table 3). For overall survival and patients who did not receive trastuzumab, FISH+ was more associated with age, pathologic stage (stage II–IV), nuclear grade (grade 2–3), radiotherapy, and chemotherapy, and IHC 3+ was more associated with axillary dissection, histologic grade (grade 2–3), negative hormonal receptor status, endocrine therapy, and overall survival. In patients who received trastuzumab, FISH+ was more associated with nuclear grade (grade 2–3), and IHC 3+ was more associated with axillary dissection and negative hormonal receptor status (Table 4).
Survival comparisons
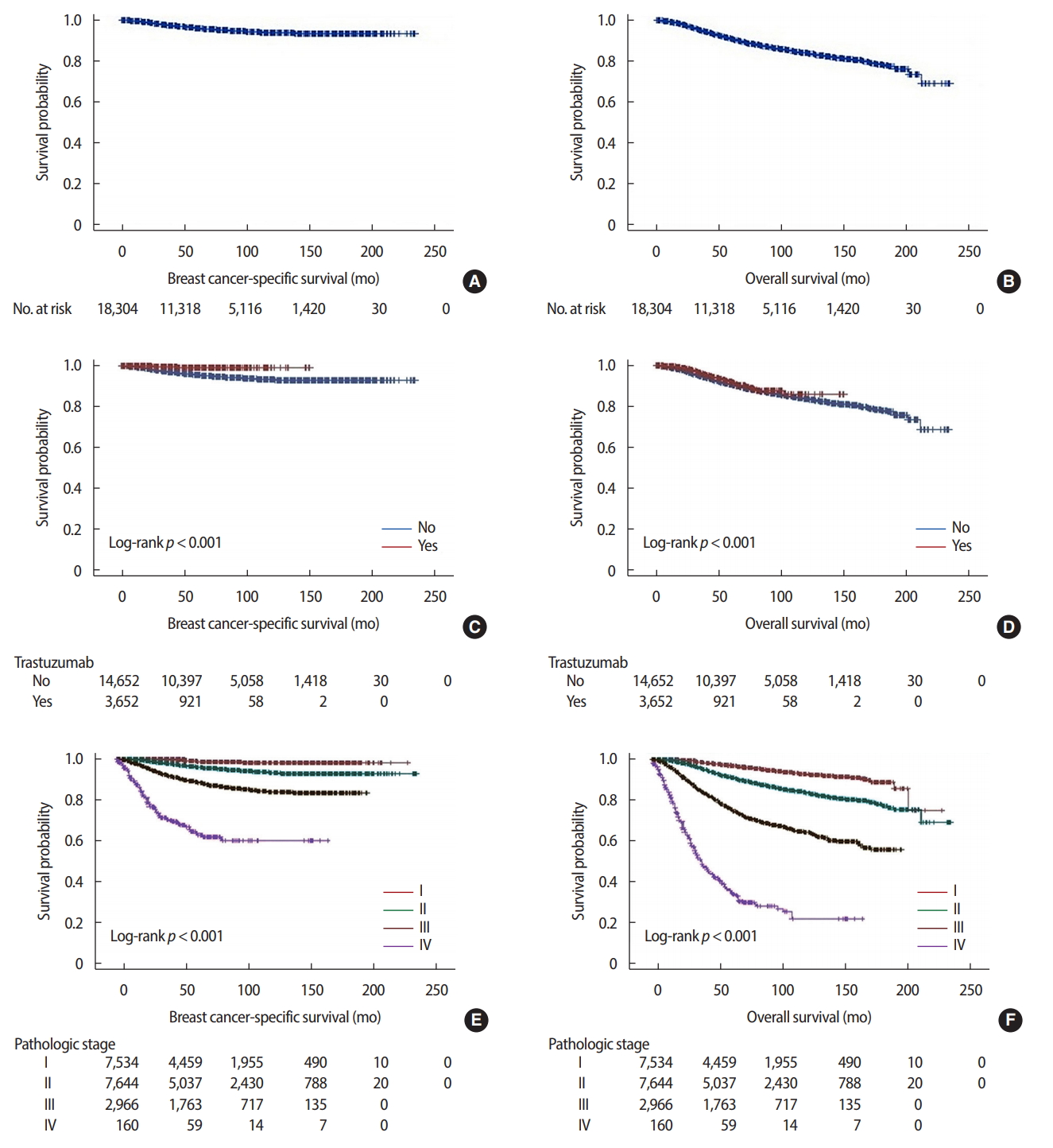
In survival comparisons using the Kaplan-Meier method, 5-year cumulative survival rates of the whole HER2 subtype cohort were 95.7% and 90.8% for breast cancer-specific survival and overall survival, respectively. According to the presence or absence of trastuzumab treatment, 5-year cumulative survival rates were 99.1% and 95.2% for breast cancer-specific survival and 94.3% and 90.3% for overall survival, respectively. The HER2 subtype cohort was significantly different according to the pathologic stage in both breast cancer-specific survival and overall survival (Figure 2).
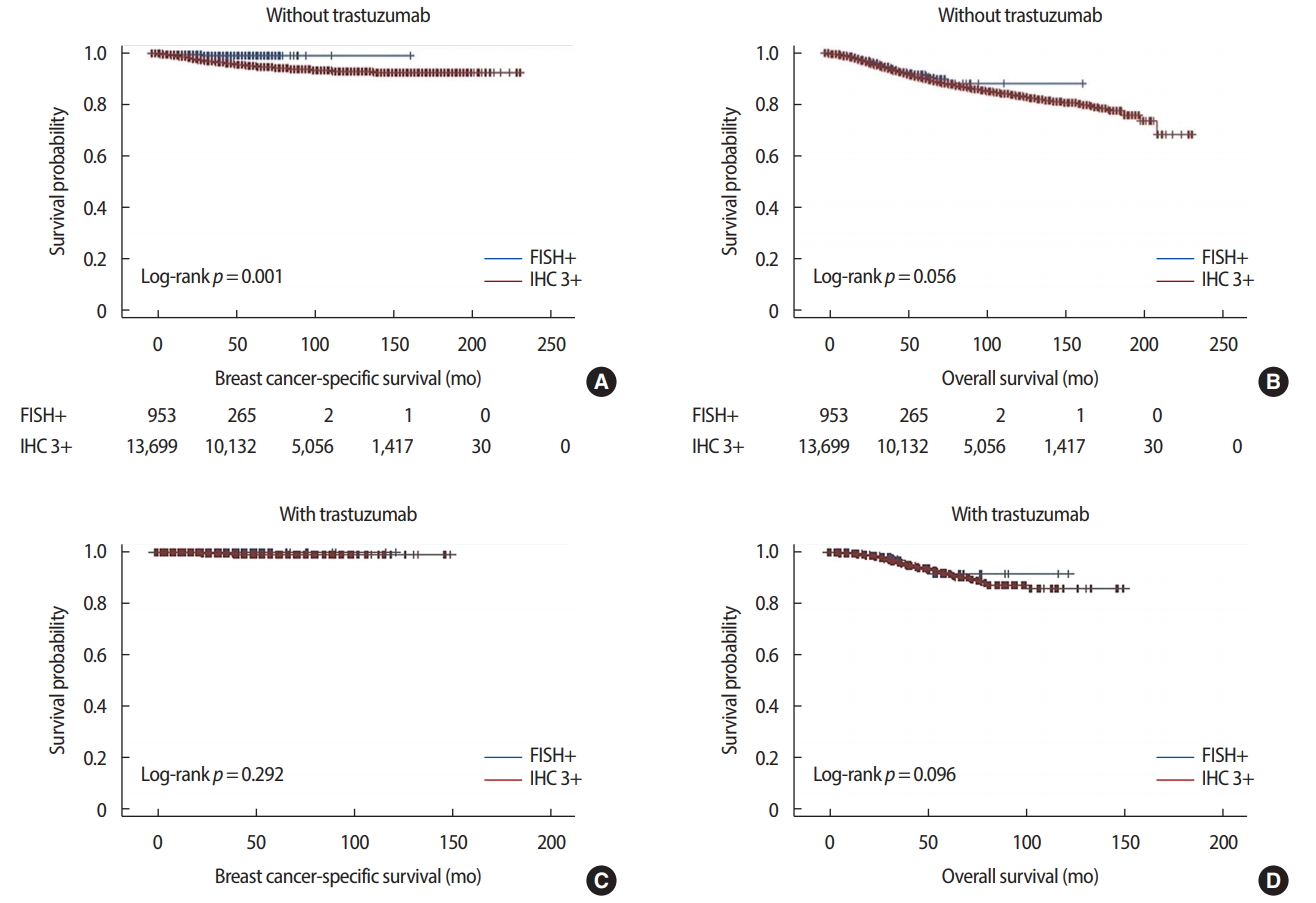
Breast cancer-specific survival was significantly different between IHC 3+ and FISH+ patients. In patients who did not receive trastuzumab, 5-year cumulative survival rates were 95.0% for IHC 3+ and 98.5% for FISH+ patients (p = 0.001). In patients who received trastuzumab, 5-year cumulative survival rates were 99.1% for IHC 3+ and 100.0% for FISH+ (p = 0.292). There was no difference in overall survival rates between the IHC 3+ and FISH+ groups, either with or without trastuzumab treatment (Figure 3). In Cox proportional hazard models, depending on the presence or absence of trastuzumab use, the factors affecting breast cancer-specific survival were age (hazard ratio [HR], 1.023, p = 0.011), mastectomy (HR, 1.989, p< 0.001), axillary dissection (HR, 4.006, p< 0.001), pathologic stage (stage II: HR, 2.648, p< 0.001; stage III: HR, 6.753, p< 0.001; stage IV: HR, 14.921, p < 0.001), histologic grade (grade 3: HR, 2.053, p = 0.041), nuclear grade (grade 2: HR, 0.534, p = 0.012; grade 3: HR, 0.598, p = 0.029), and chemotherapy (HR, 0.586, p = 0.007) in patients who did not receive trastuzumab, and none in patients who received trastuzumab (Table 5). Factors affecting overall survival were mastectomy (HR, 1.653, p< 0.001), axillary dissection (HR, 1.838, p< 0.001), pathologic stage (stage II: HR, 2.543, p< 0.001; stage III: HR, 6.159, p< 0.001; stage IV: HR, 13.390, p< 0.001), histologic grade (grade 2: HR, 1.518, p = 0.038; grade 3: HR, 1.816, p = 0.004), and chemotherapy (HR, 0.490, p< 0.001) in patients who did not receive trastuzumab, while pathologic stage (stage III: HR, 6.012, p = 0.004; stage IV: HR, 228.381, p< 0.001), negative hormonal receptor status (HR, 3.169, p = 0.005), and endocrine therapy (HR, 2.216, p = 0.040) affected overall survival in patients who received trastuzumab (Table 6).
DISCUSSION
Implicated in the growth of breast cancer, the HER2 receptor has become a target for breast cancer therapy. Since the discovery of the HER2/neu oncogene, FISH has helped overcome the diagnostic ambiguity of the existing IHC method for determining HER2 positivity [19,20]. HER2 gene amplification in FISH is more than 90% identical to HER2 receptor protein overexpression, and HER2 positivity is related to prognosis. However, in some cases, there may be overexpression of the HER2 receptor without HER2 gene amplification, and vice versa, leading to inconsistent results [21]. Although FISH is used as a gold standard for measuring HER2/neu gene amplification, SISH has been shown to be as feasible as FISH to determine HER2 status in some recent studies [22].
Correlations between these two diagnostic methods in HER2-positive breast cancer differ from study to study. Petroni et al. [12] reported that HER2-positive breast cancer showed unfavorable features in patients exhibiting gene amplification in FISH, even though the HER2 protein was expressed at lower amounts. Mass et al. [23] analyzed three clinical trials targeting overexpression in IHC 2+ or 3+ patients, and they reported that treatment of metastatic breast cancer with trastuzumab in FISH-positive patients improved response and survival rates compared to FISH-negative cancer, indicating that FISH can be an important method for diagnosis of HER2 positivity. In contrast, Toi et al. [24] reported that in patients with metastatic HER2-positive breast cancer, overall survival was significantly higher in the group with a higher degree of HER2 expression, and the effects of trastuzumab could be seen. Lipton et al. [25] reported that most HER2 IHC 3+ cases were concordant with positive FISH in 102 patients with metastatic breast cancer, and higher levels of gene amplification in FISH and HER2 protein expression in IHC were associated with a relatively longer time to progression. Additionally, FISH positive cases with low HER2 protein expression have a similar prognosis to FISH negative cases with low HER2 protein expression.
There are also studies where the results of these two methods do not vary. Zabaglo et al. [13] reported that in the Herceptin Adjuvant (HERA) trial of early-stage breast cancer patients, HER2 staining intensity and FISH amplification had a positive correlation, independent of the degree of HER2 staining intensity; however, disease-free survival was similar in both the presence and absence of trastuzumab. Xu et al. [26] reported that the HER2 amplification level was not an effective prognostic factor, finding no significant difference in disease-free survival based on a meta-analysis of trastuzumab use in HER2 positive patients.
We observed a difference between the IHC 3+ and FISH+ groups in relation to other clinical factors. When analyzed according to the presence or absence of trastuzumab, FISH+ was mainly associated with nuclear grade, and IHC 3+ was mainly associated with axillary dissection and negative hormonal receptor status. Nuclear grade is associated with chromosome 17 polysomy in relation to FISH positivity. Chibon et al. [27] compared ASCO/CAP and FDA guidelines, finding that the HER2/CEP17 ratio was associated with mitotic count and nuclear atypia. In relation to survival factors, although IHC 3+ group was more associated with breast cancer-specific survival and overall survival than FISH+ group and a worse survival curve of breast cancer-specific survival in the absence of trastuzumab, survival differences between the two groups were not significant in Cox proportional hazard models. It is thought that other factors associated with IHC 3+ or FISH+ probably affected survival as confounding factors. Further evaluation is needed for clinical factors, such as histologic subtypes, not included in the existing analysis.
In this study, the usage rate of trastuzumab was lowered to 18.7% in the IHC 3+ group and 34.5% in the FISH group. The reasons for the low usage rates are the high proportion of early breast cancer in this study and the possibility of missing data, which is an inborn limitation of retrospective analyses. In South Korea, trastuzumab has been approved since 2003. Approval criteria are lymph node positive or tumor size greater than 1 cm. The difference in use of trastuzumab before and after the approval was 0.3% versus 21.8% in the IHC 3+ group and 0% versus 34.6% in the FISH+ group.
This study does have several limitations, including the retrospective design. Although we used large-scale data, such data were passively obtained from medical records at multiple medical institutions, leading to heterogeneity and missing data. Further, only the presence or absence of HER2 amplification in FISH using the input system could be identified, and specific criteria, such as the HER2/CEP17 ratio, could not be confirmed. Recently, there have been studies in which intrinsic subtype division using gene expression assay (such as PAM50) may be useful for therapeutic response and prognosis prediction [28]. In a typical diagnostic process for HER2, most patients do not require FISH if they have an IHC score of 3+ without FISH. Most patients with HER2 FISH assay results are patients whose breast cancers have HER2 IHC 2+ immunostaining. These patients typically have breast cancers composed of a majority of HER2-not-amplified (“FISH-negative”) breast cancers and a minority that are HER2-amplified (“FISH-positive”) breast cancers. Characteristically, only modest levels of HER2 gene amplification are associated with IHC 2+ breast cancers. In contrast, the IHC 3+ breast cancers typically have higher levels of HER2 gene amplification. In comparison, relatively few of these IHC 3+ breast cancers are expected to have modest levels of HER2 gene amplification [29,30]. It is thought that additional relevant studies are required under equivalent conditions. In addition, interpretation of IHC staining by pathologists has a subjective element, potentially introducing selection bias. Finally, there were few breast cancer-specific deaths in our cohort, making it difficult to compare detailed survival rates.
In this study, the breast cancer-specific survival and overall survival were not affected by the different two diagnostic methods of HER2-positive breast cancer in Cox proportional hazard models. A strength of this study is that we objectively evaluated no difference in survival outcome between the diagnostic methods using a large-scale dataset to overcome the limitations of previous controversial studies, such as small sample size. Further research to evaluate differences in prognosis and other characteristics according to the diagnostic methods of HER2 positivity is needed in the future.